fetching data ... 
Background: Anti-phospholipid antibodies (APLA) are typically associated with thrombosis in systemic lupus erythematosus and anti-phospholipid syndrome. However, little is know about the clinical associations of these antibodies in systemic sclerosis (SSc).
Objectives: We sought to determine the prevalence and correlates of APLA in a large cohort of patients with SSc.
Methods: Patients participating in the Australian Scleroderma Cohort Study who fulfilled the ACR or Medsger criteria for SSc, were tested for APLA (anti-cardiolipin IgM [ACA IgM], anti-cardiolipin IgG [ACA IgG] and anti-beta2 glycoprotein antibodies [Anti-β2GP]) using commercial ELISA assays at each annual visit. APLA and various clinical manifestations were defined as present ever from SSc diagnosis. Chi-square and unadjusted logistic regression were used to identify and quantify clinical associations of APLA in SSc.
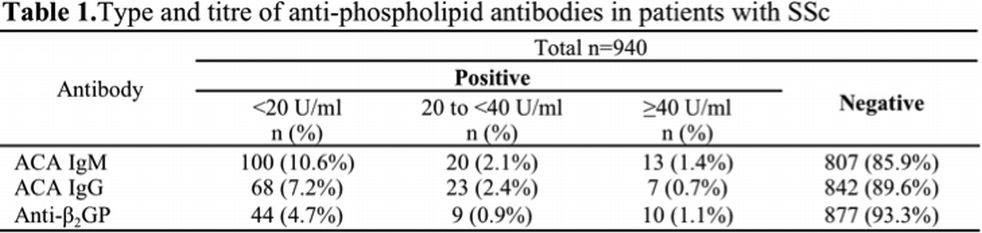
Results: One or more types of APLA were present in 226 (24.0%) of 940 patients included in the study. There were no patients with lupus anticoagulant. Type and titre of APLA are summarized in Table1. Moderate to high titre ACA IgG were associated with right heart catheter-diagnosed pulmonary arterial hypertension (PAH) (odds ratio 1.6, 95% CI: 1.03-2.52, p=0.038). Both ACA IgM (odds ratio 2.04, 95% CI: 1.4-3.0, p<0.0001) and ACA IgG (odds ratio 1.84, 95% CI: 1.2-2.8, p=0.005) were associated with interstitial lung disease (ILD). ACA IgG was a marker of coexistent PAH and ILD (odds ratio 2.10, 95% CI: 1.1-4.2, p=0.036). There was no association between APLA and SSc disease subtype (limited v. diffuse), presence of other autoantibodies, or other disease manifestations e.g. renal crisis.
Conclusions: Anti-phospholipid antibodies are found in 24% of patients with SSc, but in most cases the titres are low (<20 U/ml). Moderate to high titre APLA are associated with a 1.6 to 2-fold increased risk of PAH or ILD, and a 2-fold increased risk of coexistent PAH and ILD in SSc.
Disclosure of Interest: None Declared