fetching data ... 
Background: EULAR/ACR guidelines recommend Methotrexate (MTX) with or without glucocorticoids (GCs) for DMARD naïve patients. Triple DMARD therapy however is not recommended in these guidelines, because well proven evidence of superior efficacy is lacking. However, we recently published a superior effect after 3 months in favor of triple DMARD therapy independent of GCs. Longer follow-up was needed.
Objectives: To compare the clinical efficacy of: (1) triple DMARD therapy vs. MTX mono-therapy and (2) oral GCs bridging therapy vs. 1 dose of intramuscular (im) GCs in patients with early RA.
Methods: The one-year data of the ongoing single-blinded randomized clinical trial in patients with recent-onset arthritis (tREACH) were used. All patients, who had a high probability (>70%) of progressing to persistent arthritis, based on the prediction model of Visser, were included. At baseline 267 (95%) of patients fulfilled the 2010 criteria for RA. Patients were randomized into 3 induction therapy strategies: (A) triple DMARD therapy (MTX 25 mg + Sulphasalazine 2 gr. + Hydroxychloroquine 400 mg) with im GCs (Depomedrol 120mg), (B) triple DMARD therapy with an oral GCs tapering scheme (starting 15 mg) and (C) MTX 25 mg with oral GCs similar to B. Treatment strategies were ‘tightly controlled’, with patients being examined every 3 months. Treatment decisions were based upon the original DAS threshold for low disease activity. We investigated DAS and HAQ response over time, using a linear mixed model (LMM).
Results: A total of 281 patients were included and randomly assigned to A (n=91), B (n=93) or C (n=97). Patients were mostly females (68%) with an average symptom duration of 166 days (95% CI: 156 – 177). At baseline 216 (77%) patients were ACPA positive and 48 (16%) patients had erosions. Despite randomization, symptom duration, occurrence of erosions and proportion of patients fulfilling 1987 criteria for RA differed significantly between treatment arms. Figure 1 shows the HAQ and DAS per treatment arm over time. At three months a statistical superior effect was seen favouring triple DMARD therapy. In our LMM there is no significant difference in DAS and HAQ between triple DMARD therapy and MTX mono-therapy after 12 months (β=-0.15, p=0.056 and β=-0.052, p=0.28 respectively). However after correction for baseline differences, DAS differed significantly after 12 months of therapy in favour of the triple DMARD therapy (β=-0.16, p=0.044). There were no differences in HAQ and DAS after 12 months between both GCs bridging therapies.
Image/graph:
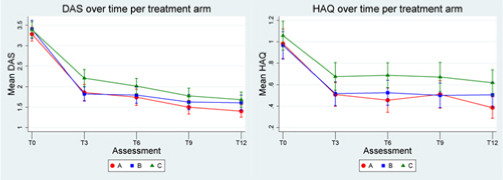
Conclusions: In patients with early RA triple DMARD therapy stays superior to MTX mono-therapy even after 12 months of therapy. Furthermore both intramuscular and oral GCs can be used as bridging therapy.
Disclosure of Interest: None Declared