fetching data ... 
Background: Biologic DMARDs (bDMARDs) are used to treat patients (pts) with moderate to severe rheumatoid arthritis (RA). Pts may experience clinical benefits from treatment with bDMARDs alone or with a conventional synthetic DMARD (csDMARD).
Objectives: To assess treatment patterns and healthcare resource use (HCRU) after prescription/administration of a bDMARD alone or with a csDMARD.
Methods: In this retrospective cohort analysis, pts aged ≥18 years (yrs) with an RA diagnosis (ICD9: 714.xx) who were prescribed/administered a DMARD (2007–2011) were selected from de-identified US electronic health records (EHR; Humedica). Index date was date of first prescription/administration for a bDMARD (adalimumab, certolizumab, etanercept, golimumab, infliximab, rituximab, anakinra, tocilizumab). Pts did not receive bDMARDs for ≥6 months pre-index and were followed for ≥1 yr post-index. Pts were classified by index biologic monotherapy (Bmono) or combination therapy with bDMARD and csDMARD (B+CScombo; based on methotrexate, leflunomide, sulfasalazine, hydroxychloroquine at index). Regression analyses for switch (new bDMARD/csDMARD prescription/administration and no index drug for ≥120 days) and RA-related costs were assessed controlling for differences in pt demographics/characteristics. RA-related costs were derived from a pt subset with linked Optum claims data and applied to RA visits and pharmacy use in EHR.
Results: Of 2119 pts initiating a bDMARD, 70.6% received Bmono and 29.1% received B+CScombo; 0.2% had ≥2 biologics. Pt characteristics and treatment patterns are presented in Table 1. Mean age and percentage of females were similar for Bmono and B+CScombo pts. Compared with B+CScombo pts, Bmono pts were more likely to be treated by a rheumatologist, had a higher Deyo-Charlson Co-morbidity Index score and were more likely to have cardiovascular disease, hyperlipidaemia, hypertension and renal disease. Most Bmono and B+CScombo pts were prescribed a TNF inhibitor (TNFi). During 1-yr follow-up (FU), B+CScombo pts were less likely to switch index regimen vs Bmono pts (OR 0.37; 95% CI 0.27, 0.51; p<0.0001). More than one-third of Bmono pts switched index regimen, with most switching to a csDMARD. A small proportion of B+CScombo pts switched index regimen with more than half switching the bDMARD of the B+CScombo regimen and the remainder switching the csDMARD of the B+CScombo regimen. Compared with Bmono pts, B+CScombo pts had lower mean RA-related office and outpatient visits but more prescriptions. Adjusted total RA-related costs were 30% lower for Bmono vs B+CScombo pts.
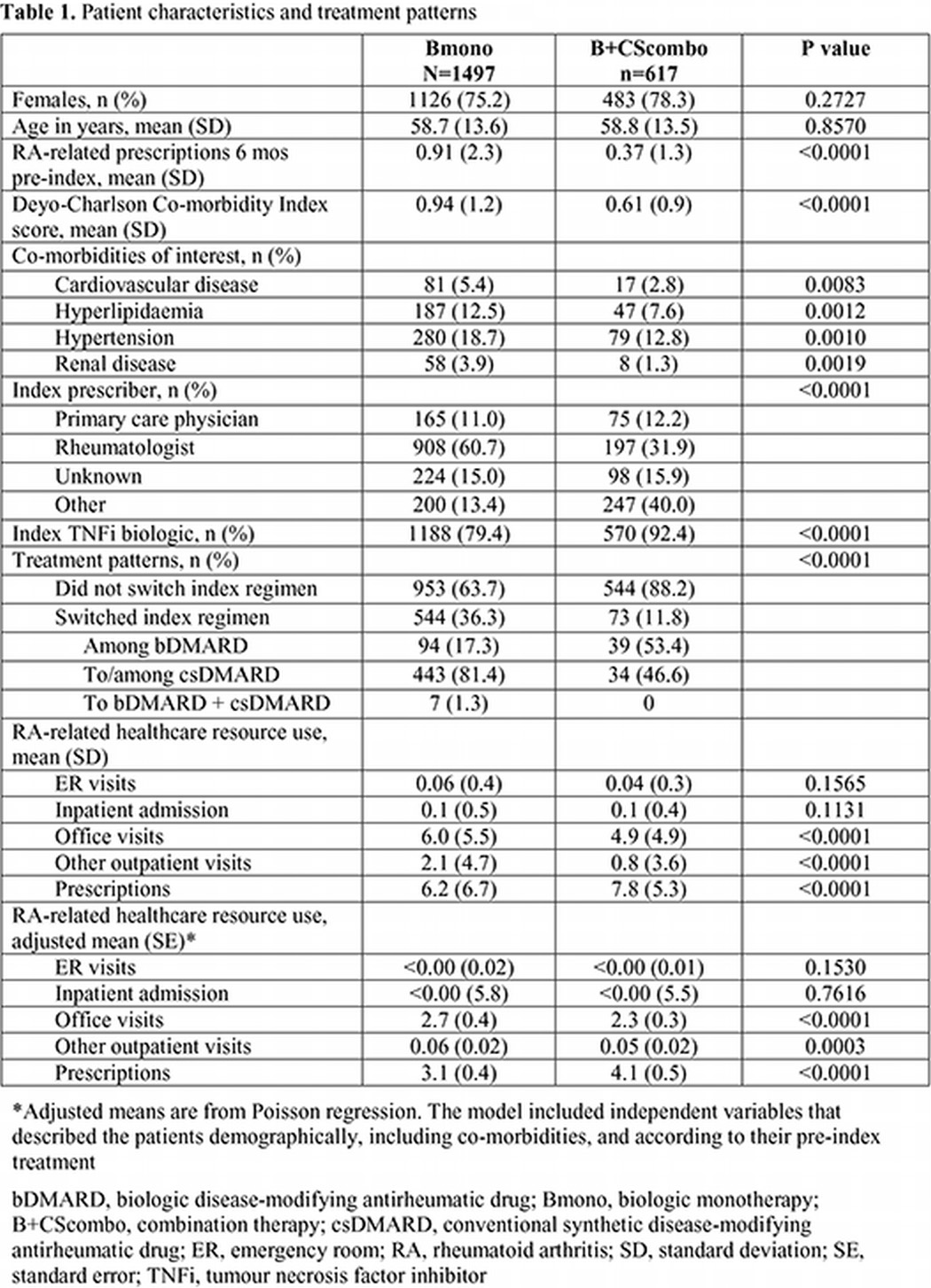
Conclusions: In this analysis of EHR data characterising bDMARD prescriptions/administrations in pts with RA, 70.6% received Bmono, and had a greater prevalence of co-morbidities and were more likely to be treated by a rheumatologist vs B+CScombo pts. B+CScombo pts were less likely to switch index regimen in 1-yr of FU and had lower RA-related medical HCRU but greater total costs vs Bmono pts. High prevalence of Bmono use may be due to a stricter concomitant csDMARD definition or the data source, which included specialties other than rheumatology.
Acknowledgements: This study was sponsored by Pfizer Inc. Editorial Support was provided by Karen Irving at Complete Medical Communications and funded by Pfizer Inc.
Disclosure of Interest: J. Harnett Shareholder of: Pfizer Inc., Employee of: Pfizer Inc., R. Gerber Shareholder of: Pfizer Inc., Employee of: Pfizer Inc., D. Gruben Shareholder of: Pfizer Inc., Employee of: Pfizer Inc., D. Wiederkehr Shareholder of: Pfizer Inc., Employee of: Pfizer Inc., E. Mahgoub Shareholder of: Pfizer Inc., Employee of: Pfizer Inc., G. Wallenstein Shareholder of: Pfizer Inc., Employee of: Pfizer Inc., A. Koenig Shareholder of: Pfizer Inc., Employee of: Pfizer Inc.
DOI: 10.1136/annrheumdis-2015-eular.3650