fetching data ... 
Background: Reducing psoriasis burden in subjects with active PsA and concomitant psoriasis is an important aspect of disease management. The randomized, double-blind, placebo (PBO)-controlled phase 3 FUTURE 2 study (NCT01752634) demonstrated that secukinumab, a human anti–IL-17A monoclonal antibody, significantly improved the signs and symptoms of active psoriatic arthritis (PsA) and provided an opportunity to evaluate the impact on skin disease burden.1
Objectives: To evaluate the effects of subcutaneous (s.c.) secukinumab on dermatologic parameters in the FUTURE 2 study.
Methods: 397 adults with active PsA were randomized to s.c. secukinumab (300, 150 or 75 mg) or PBO at baseline, Wk 1, 2, 3, 4 and then every 4 wks thereafter. The primary endpoint was American College of Rheumatology 20 (ACR20) response at Wk 24. Assessments of psoriasis burden included ≥75% and ≥90% improvement in Psoriasis Area and Severity Index (PASI 75/90). The primary endpoint and PASI 75/90 secondary endpoints were included in a hierarchical testing analysis and were adjusted for multiplicity at Wk 24. Other assessments were exploratory endpoints. Exploratory skin assessments were Investigator's Global Assessment (modified 2011) score of 0 or 1 (IGA 0/1), and the Dermatology Life Quality Index (DLQI). All skin assessments were undertaken in patients (pts) with psoriasis affecting ≥3% of body surface area. Effect of treatment on modified Nail Psoriasis Severity Index (mNAPSI) was assessed in pts with nail involvement. The effect of treatment on the inflammatory marker high-sensitivity C-reactive protein (hsCRP) was monitored in all pts.
Results: At Wk 24, PASI 75/90 response rates were significantly improved with secukinumab 300 and 150 mg vs PBO (Table). Secukinumab also improved IGA 0/1 and mNAPSI scores, reduced hsCRP levels and provided clinically meaningful improvement (≥4-point change from BL) in DLQI vs PBO at Wk 24 (Table).
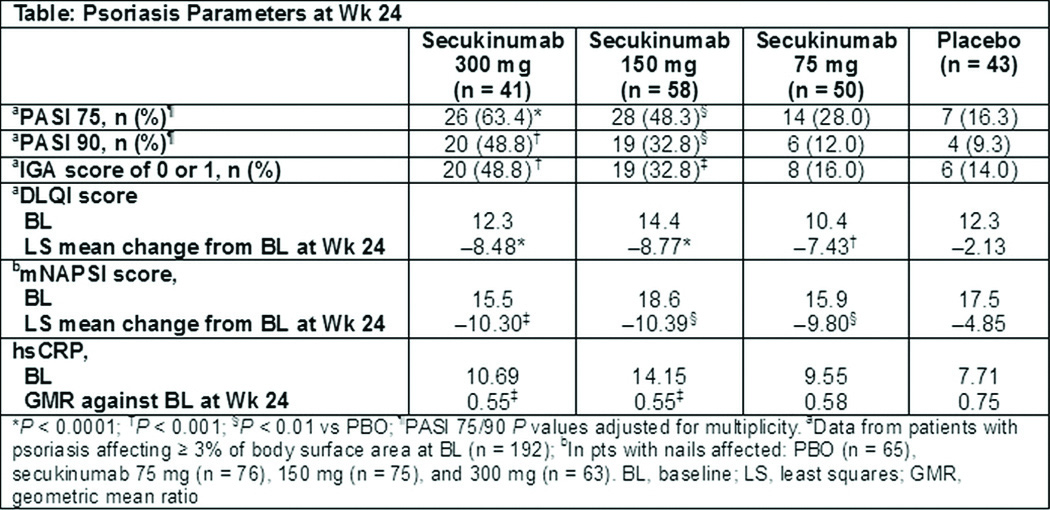
Conclusions: Secukinumab 300 and 150 mg s.c. reduced the severity of plaque and nail psoriasis and improved skin-related quality of life in subjects with active PsA and significant concomitant psoriasis burden.
References:
1. McInnes IB, et al. Presented at ACR 2014; L1
Acknowledgements: Medical writing support was provided by Rachel Mason at Seren Communications (Tytherington, UK), and was funded by Novartis.
Disclosure of Interest: A. Gottlieb Grant/research support from: Centocor (Janssen), Amgen, Abbott (Abbvie), Novartis, Celgene, Pfizer, Lilly, Coronado, Levia, Merck, and Xenoport, Consultant for: Amgen Inc., Astellas, Akros, Centocor (Janssen), Inc. Celgene Corp., Bristol-Myers Squibb Co., Beiersdorf, Inc., Abbott Labs. (Abbvie), DUSA, TEVA, Actelion, UCB, Novo Nordisk, Novartis, Dermipsor Ltd., Incyte, Pfizer, Canfite, Lilly, Coronado, Vertex, Karyopharm, CSL Behring Biotherapies for Life, GlaxoSmithKline, Xenoport, Catabasis, and Sanofi-Aventis, I. McInnes Consultant for: Novartis, Amgen, Janssen, BMS, Pfizer, UCB, Abbvie, Celgene, and Lilly, P. Mease Grant/research support from: AbbVie, Amgen, Biogen Idec, BMS, Celgene, Crescendo, Janssen, Lilly, Merck, Novartis, Pfizer, UCB, and Vertex, Consultant for: AbbVie, Amgen, Biogen Idec, BMS, Celgene, Covagen, Crescendo, Janssen, Lilly, Merck, Novartis, Pfizer, UCB, and Vertex, Speakers bureau: AbbVie, Amgen, Biogen Idec, BMS, Crescendo, Janssen, Lilly, Pfizer, and UCB, P. Rahman Consultant for: Abbott, AbbVie, Amgen, BMS, Celgene, Janssen, Novartis, Pfizer, and Roche. Consultant to pharmaceutical companies dealing with biologic agents in rheumatology, S. Kandala Employee of: Novartis, M. Patekar Employee of: Novartis, S. Mpofu Shareholder of: Novartis, Employee of: Novartis
DOI: 10.1136/annrheumdis-2015-eular.2852