fetching data ... 
Background: Guidelines support the use of combination conventional synthetic Disease-Modifying Antirheumatic Drugs (csDMARDs), switching csDMARDs and/or use of biologic DMARDs (bDMARDs) treatment in active rheumatoid arthritis (RA) after use of methotrexate (MTX).
Objectives: The purpose of this study was to determine treatment practices after use of MTX in patients with RA who were on either monotherapy or combination csDMARDs in a large observational cohort (OBRI) in order to determine contemporary practice where use of bDMARDs from government coverage is restricted to active RA (+RF and/or +ACPA) or erosions, SJC≥5 with MTX failure, combination failure (triple csDMARDs: MTX + hydroxychloroquine + sulfasalazine) or use of leflunomide.
Methods: Patients enrolled in OBRI with documented MTX failure defined as discontinuation due to side effect, primary/secondary failure, or patient/physician decision. Demographics and disease parameters at MTX failure were compared between monotherapy failures, double therapy (Rx) failures, and triple Rx failures.
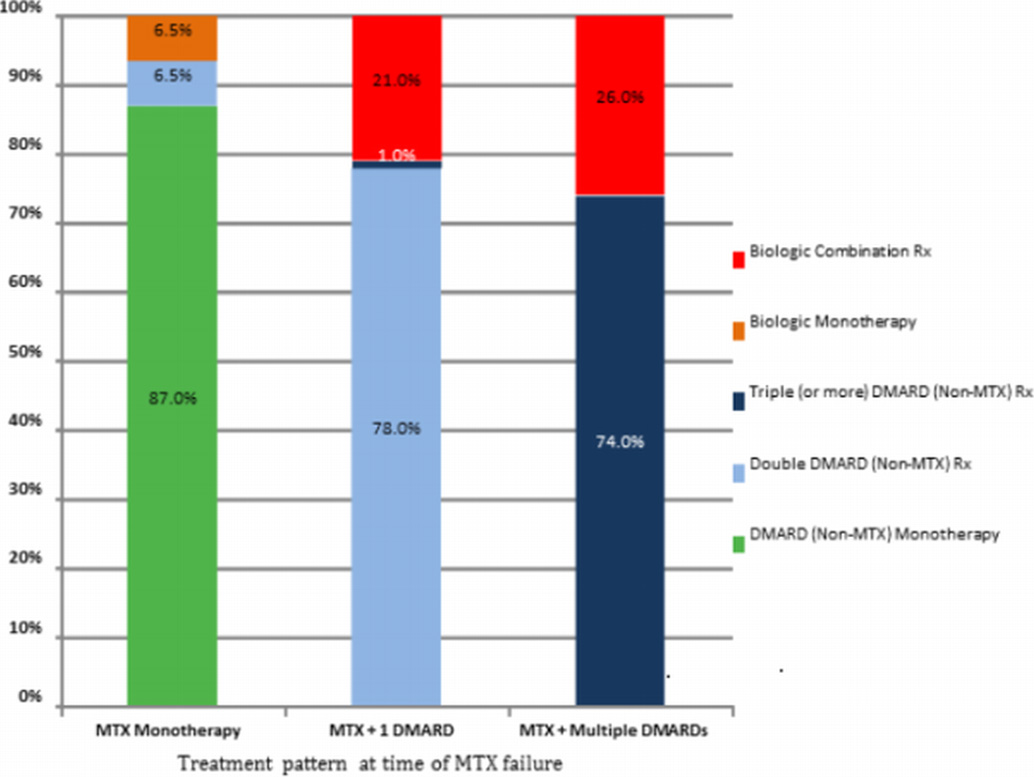
Results: A total of 313 patients with MTX failure were included with a mean (SD) age of 58.8 (13.2) years and disease duration of 6.7 (8.2) years. Of these, 102 (32.6%) were on MTX monotherapy, 156 (49.8%) were double (MTX +1 csDMARD) Rx, and 55 (17.6%) were on triple or more (MTX + multiple csDMARDs)Rx, respectively, at the time of MTX failure. At the time of MTX failure disease duration was numerically higher in patients failing monotherapy and double Rx as compared to triple Rx (7.5 vs. 6.8 vs. 4.5 years, respectively; P=0.276) while patients failing triple Rx were more likely to have an erosion (43.1% vs. 37.2% vs. 61.8%; P=0.009) and had significantly higher patient global (3.5 vs. 3.9 vs. 4.8; P=0.046). When looking at patient transition to csDMARDs monotherapy, csDMARDs combination Rx or bDMARDs treatment, patients receiving monotherapy were more apt to have switches to other monotherapy (87% of patients), whereas those on combination Rx received more combination csDMARDs (78% and 74% of patients on MTX + 1 csDMARDs or MTX + multiple csDMARDs, respectively) and bDMARDs combination Rx (21% and 26%, respectively)(Figure 1).
Figure 1. Treatment profile after MTX failure by type of MTX failure
Conclusions: There are inherent differences in the selection of subsequent treatment regimen between patients failing MTX monotherapy vs. MTX combination therapy. Overall, the results of the current analysis suggest the use of a sequential treatment intensification strategy in routine clinical practice in Ontario.
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2016-eular.4199