fetching data ... 
Background: Antiphospholipid antibodies (aPL) are risk factors for Adverse Pregnancy Outcome (APO). The therapeutic strategy to adopt in aPL patients during pregnancy should in fact consider different clinical and serological risk factors. In addition to conventional therapy, some recent evidences suggest a possible role of hydroxychloroquine.
Objectives: To review our approach in first-line treated pregnancies in aPL patients in our 30 years' experience Pregnancy Clinic (1985 -2015) to find out which clinical and serological risk factors have influenced the choice of treatments and which should be considered in the future for possible additional treatments.
Methods: We reviewed 120 first-treated pregnancies that were prospectively followed in our center by a multispecialistic team of Rheumatologists and Obstetricians. Patients were classified as Primary Antiphospholipid Syndrome (PAPS) according to revised criteria and as Incomplete PAPS or aPL carriers according to their clinical history or aPL status. Patients with concomitant systemic autoimmune diseases were excluded. aPL profile was defined as the combination of the 3 criteria tests for aPL (Lupus Anticoagulant, anti-cardiolipin, anti-Beta2 Glycoprotein I). APO was defined as at least one of the followings: miscarriage (<10th week), fetal death (≥10th week), severe preterm delivery (≤34th week) with or without preeclampsia (PE), HELLP syndrome or perinatal death.
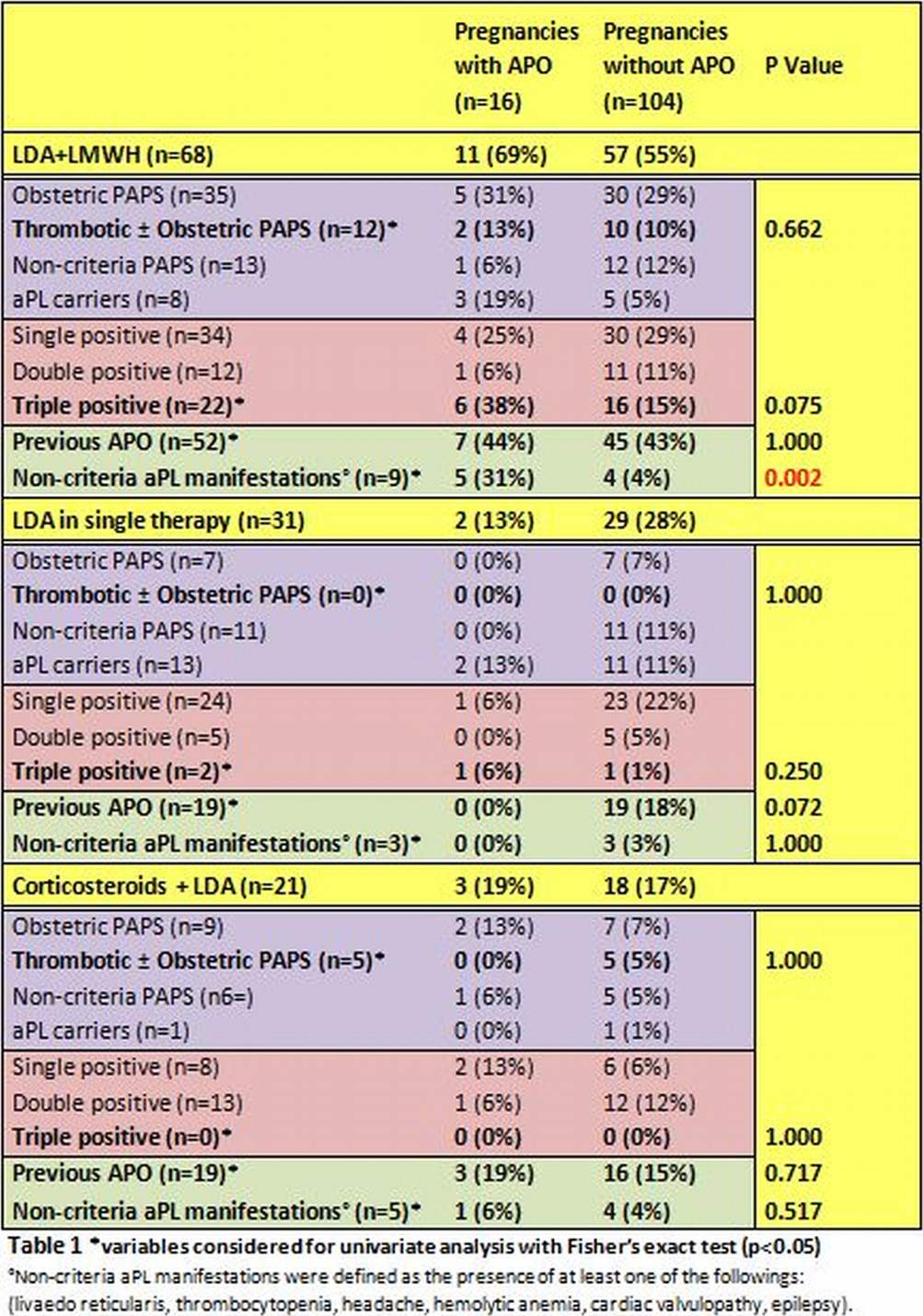
Results: The type of therapy was divided in three main categories: combination therapy with low molecular weight heparin (LMWH) and LDA (68,57%), single therapy with low dose aspirin (LDA) (31,26%) and therapy with corticosteroids plus LDA (21,18%).
We collected 16 APO (13%): 11 (75%) in the category of LMWH+LDA. Analyzing APO vs. non-APO pregnancies we found no differences in variables that could predict an APO (history of thrombosis, a previous APO or a triple positive aPL profile) in any of the 3 categories (Table 1). Moreover, we found an increased rate of non criteria aPL manifestations in APO patients in LMWH+ASA category (31% vs. 4%, p:0.002; OR 2.19, 95%CI 2.20–61.6), but not in the other 2 categories of treatment.
Conclusions: Non-criteria aPL manifestations are a risk factor for APO ande can determine failure to conventional treatment with LMWH plus LDA during pregnancy in aPL patients regardless of clinical diagnosis, serological profile or obstetric history. These patients may represent a more severe phenotype of disease and may deserve an immunomodulatory treatment to increase the probability of success during pregnancy.
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2016-eular.4593