fetching data ... 
Background: One of the primary aims for children and young people with JIA is remission. Early improvement in disease likely predicts greater chance of remission in the longer-term.
Objectives: To assess the association between change in disease activity over the first year of disease and later occurrence of remission.
Methods: Children and young people with oligoarticular, RF-negative or RF-positive polyarticular JIA recruited to the Childhood Arthritis Prospective Study prior to January 2014 were selected for analysis.
Two definitions of remission based on clinically inactive disease at two consecutive study follow-ups were explored: 1) Wallace’s preliminary criteria and 2) the clinical Juvenile Arthritis Disease Activity Score in 10 joints (cJADAS10). Association between changes in JIA core outcome variables and pain over the first year of disease and later occurrence of remission were analysed using logistic regression models, adjusting additionally for age, gender, symptom duration and predictor value at presentation. Oligoarticular and polyarticular JIA were modelled separately. Multiple imputation accounted for missing data.
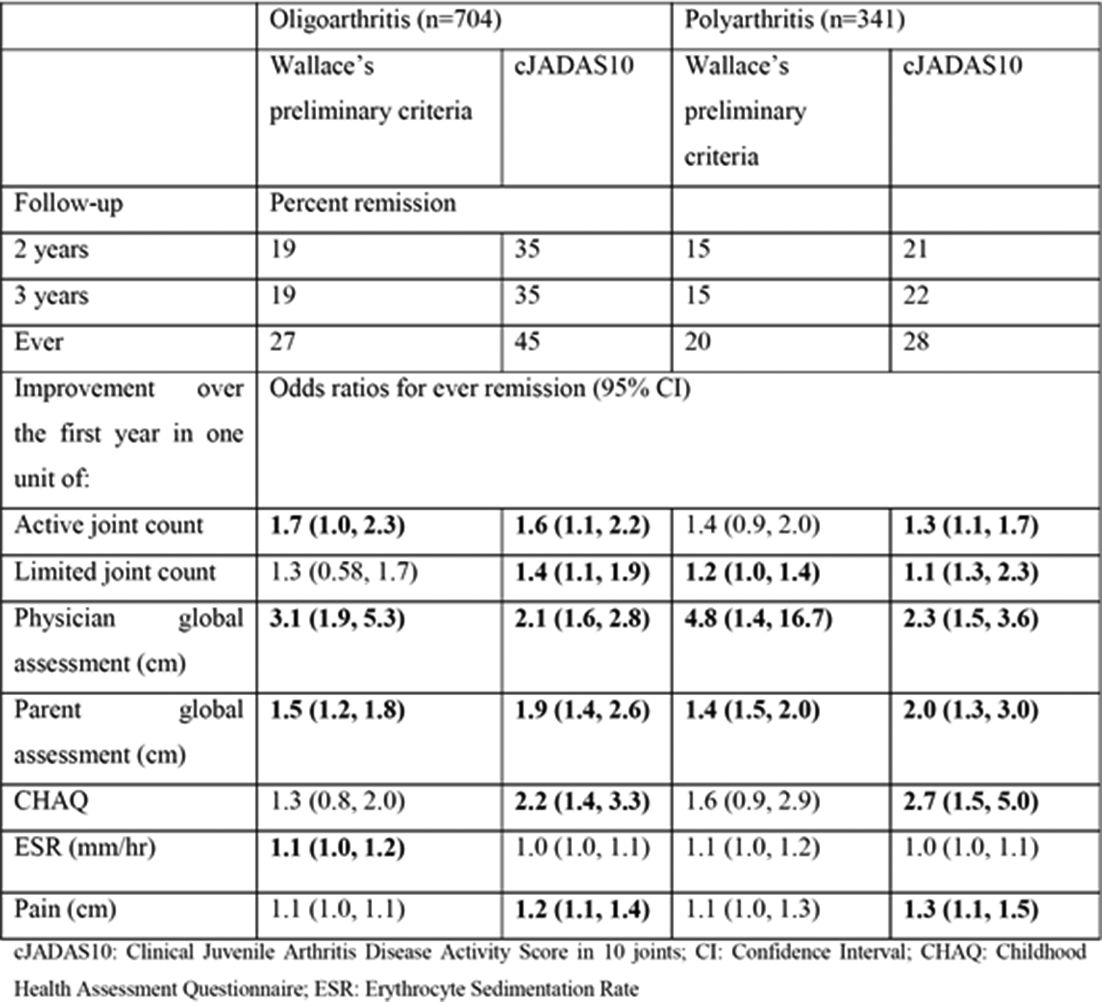
Results: A total of 1045 children were included. Of these, 70% were female and the majority had oligoarticular JIA (67%). The median age at presentation was 7 years (IQR 3, 11). Within three years, 25% achieved remission according to Wallace’s criteria and 39% according to cJADAS10. More children with oligoarticular JIA achieved remission than those with polyarticular JIA (table 1).
Remission using Wallace’s criteria was predicted in oligo and polyarthritis respectively by improvements in physician’s global (OR: 3.1, 95% CI: 1.9 to 5.3; OR: 4.8, 95% CI: 1.4 to 16.7) and parental global (OR: 1.5, 95% CI: 1.2 to 1.8; OR: 1.4, 95% CI: 1.5 to 2.0). For oligoarthritis, additional predictors included improvement in active joint count (OR: 1.7, 95% CI: 1.0 to 2.3) and ESR (OR: 1.1, 95% CI: 1.0 to 1.2). Improvement in limited joint count also predicted remission in polyarticular JIA (OR: 1.2, 95% CI: 1.0 to 1.4) (table 1).
Remission using cJADAS10 was predicted in oligo and polyarthritis respectively by improvements in physician’s global (OR: 2.1, 95% CI: 1.6 to 2.8; OR: 2.3, 95% CI: 1.5 to 3.6), parental global (OR: 1.9, 95% CI: 1.4 to 2.6; OR: 2.0, 95% CI: 1.3 to 3.0), active joint count (OR: 1.6, 95% CI: 1.1 to 2.2; OR: 1.3, 95% CI: 1.1 to 1.7), limited joint count (OR: 1.4, 95% CI: 1.1 to 1.9; OR: 1.1, 95% CI: 1.3 to 2.3), CHAQ (OR: 2.2, 95% CI: 1.4 to 3.3; OR: 2.7, 95% CI: 1.5 to 5.0) and pain (OR: 1.2, 95% CI: 1.1 to 1.4; OR: 1.3, 95% CI: 1.1 to 1.5) (table 1).
Abstract OP0099 – Table 1 Achievement and predictors for remissinon according to wallace’s preliminary criteria and the cJADAS10
Conclusions: Both improvements in the physician’s and parental global assessments over the first year of disease predict remission in JIA. However, improvements in function and pain predict higher odds of remission on the cJADAS10 but not Wallace’s preliminary criteria. These factors may be helpful in predicting wellbeing but not a lack of inflammation.
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.3659