fetching data ... 
Background: PsA is a heterogeneous inflammatory arthritis. Patients (pts) with PsA suffer from associated cardiovascular disease, obesity, metabolic syndrome, diabetes (DM), osteoporosis. In psoriasis, leptin has been shown to stimulate keratinocyte proliferation, expression of adhesion molecules and angiogenesis.
Objectives: To detect the presence of premature atherosclerosis in PsA pts, measure HOMA-IR as a reflection of insulin resistance (IR) and serum leptin (LEP) level & to detect their association with the presence of premature atherosclerosis in PsA pts.
Methods: 45 PsA pts (classified according to CASPAR Criteria) & 45 healthy subjects as controls were included. Pts were subjected to history taking, clinical examination to determine body mass index (BMI), the clinical type of PsA, distribution, involved body surface area (BSA), measuring the Psoriasis Area and Severity Index (PASI) and Disease Activity in PSoriatic Arthritis: DAPSA score. Routine laboratory, fasting insulin (FI), fasting blood glucose (FBG) to calculate HOMA-IR,total cholesterol (TC), HDL, LDL, Triglycerides (TG), serum LEP, carotid Doppler to determine Carotid intima–media thickness (CIMT) & presence or absence of plaques were done. Exclusion: DM, RA, SLE, smoking, postmenopausal females, HCV infection, morbid obesity
Results: Mean BMI 22.51±1.69 and 23.46±1.82 kg/m 2 , no statistical significance (P =0.205).
Mean BSA 5.9±3.1%, DAPSA score (13.98±4.7), PASI score: 88.9% (40 pts) had mild to moderate PASI, 5 had severe disease (8.6±4.8).
TC, LDL and TG were higher in pts, while HDL was higher in controls (P =0.0003, 0.0001, 0.00001 & 0.05).
A significance between 2 groups regarding LEP (P =0.00001), ranging from 2-16.99 (9.7±4.5) in group I and 1.35-1.78 (1.6±0.1) µg/ml in controls. Normal: 2.6-8.35
FI & HOMA IR were significantly higher in PsA group (P = 0.001, 0.00001)
The mean CIMT 1.1±0.3 mm and in group II 0.8±0.1 mm. 14 pts (31.1%) had plaque, while 68.9 % & all controls had no plaques, with a significance regarding CIMT & presence of plaques (P=0.011 & 0.0041).
A positive statistical significance between LEP and dd (P=0.001), BSA, PASI and DAPSA (P =0.007, 0.003, 0.001) but not with age, BMI (P=0.98 & 0.88).
There was no statistical significance between LEP and FBG, HbA1C, HOMA IR, FI, CBC (P > 0.05), or between LEP and TC, TG, HDL, LDL (P=0.438,0.390, 0.699, 0.050), liver enzymes, renal functions, ESR and CRP.
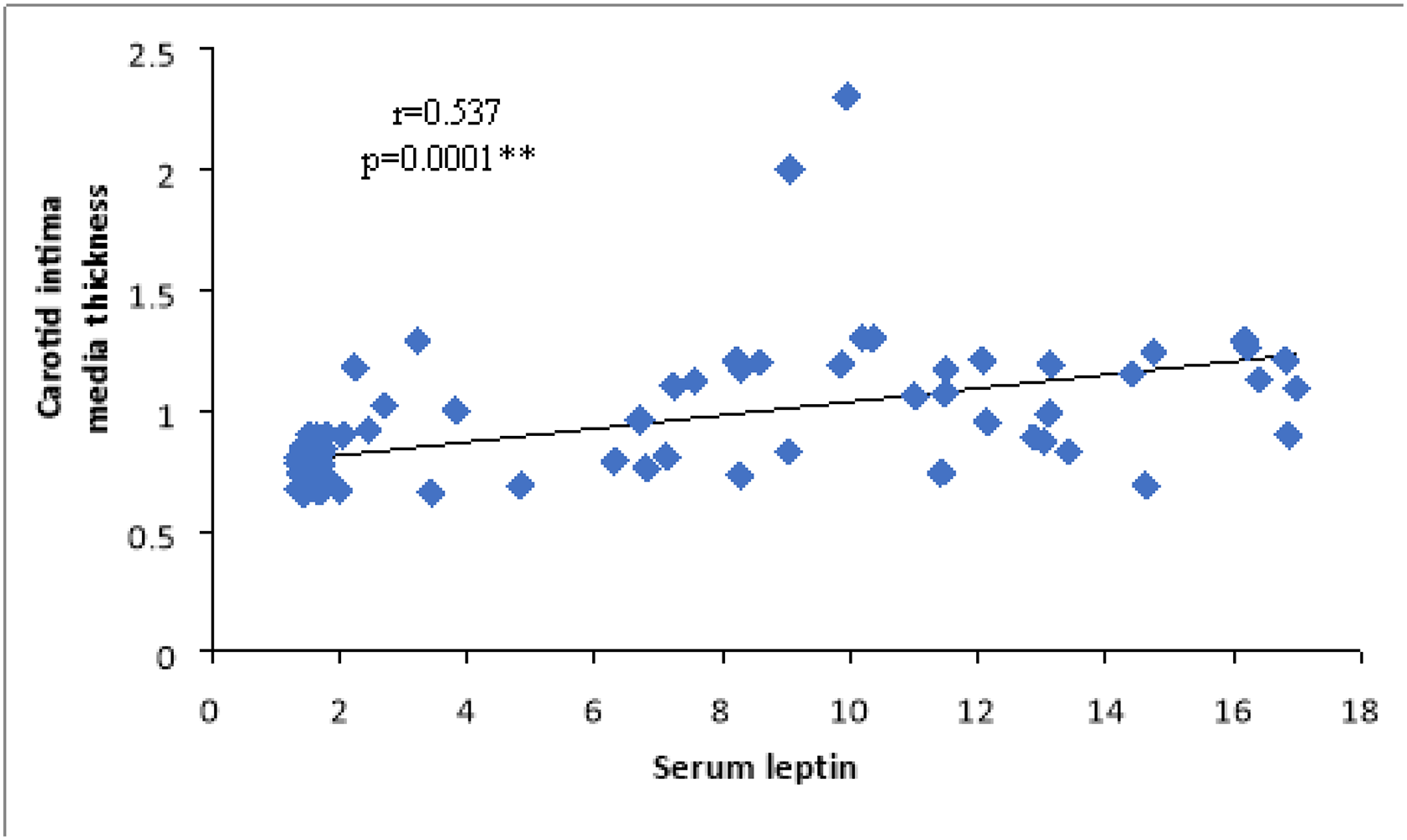
There was statistical positive correlation between LEP and CIMT (P =0.0001), but not with the presence of plaques (P=0.846).
CIMT and other variables:
DAPSA: there was no statistical significance with TC, HDL, LDL and TG (P=0.51, 0.876, 0.717 & 0.255), but a statistically significance with LEP and CIMT(p=0.001& 0.009). Pts with higher score had higher LEP and increased CIMT.
PASI: there was no significance between TC, HDL, LDL, TG (P=0.724, 0.157, 0.651& 0.374) or CIMT (p=0.290) in mild-moderate and severe PASI. LEP was significantly higher in severe PASI score (P= 0.001).
Conclusion: The presence of abnormal lipid profile, IR, increased CIMT, high disease activity and increased LEP may be considered as useful criteria for early recognition and thus prevention of atherosclerosis in PsA pts.
REFERENCES:
[1]Miller I M, et al. Meta-analysis of psoriasis, cardiovascular disease and associated risk factors. J Am Acad Dermatol 2013
| CIMT | Person correlation coefficient | p-value |
|---|---|---|
| BMI | 0.095 | 0.371 |
| Duration of disease (years) | 0.179 | 0.239 |
| BSA score | 0.12 | 0.434 |
| PASI | 0.186 | 0.221 |
| FBG | 0.059 | 0.582 |
| WBC | -0.104 | 0.329 |
| Platelet | 0.022 | 0.835 |
| Hb | -0.106 | 0.319 |
| HDL | 0.505 | 0.000** |
| LDL | 0.382 | 0.000** |
| TC | 0.275 | 0.009** |
| Triglyceride | 0.06 | 0.577 |
| SGOT | 0.03 | 0.776 |
| SGPT | 0.033 | 0.754 |
| Serum leptin | 0.537 | 0.0001** |
| HOMA IR | 0.446 | 0.000** |
| ESR | 0.351 | 0.001** |
| CRP | 0.320 | 0.002** |
| Urea | 0.445 | 0.784 |
| Creatinine | 0.392 | 0.954 |
| Uric acid | 0.034 | 0.748 |
| FI | 0.431 | 0.000** |
Disclosure of Interests: None declared