fetching data ... 
Background: Hydroxychloroquine (HCQ) and chloroquine (CQ) are effective antimalarial (AM) medications for systemic lupus erythematosus (SLE) and other autoimmune conditions such as rheumatoid arthritis (RA). AM-induced retinopathy is a well-recognized irreversible complication with variable incidences [1]. Few studies have compared the AM-induced retinopathy between rheumatologic conditions.
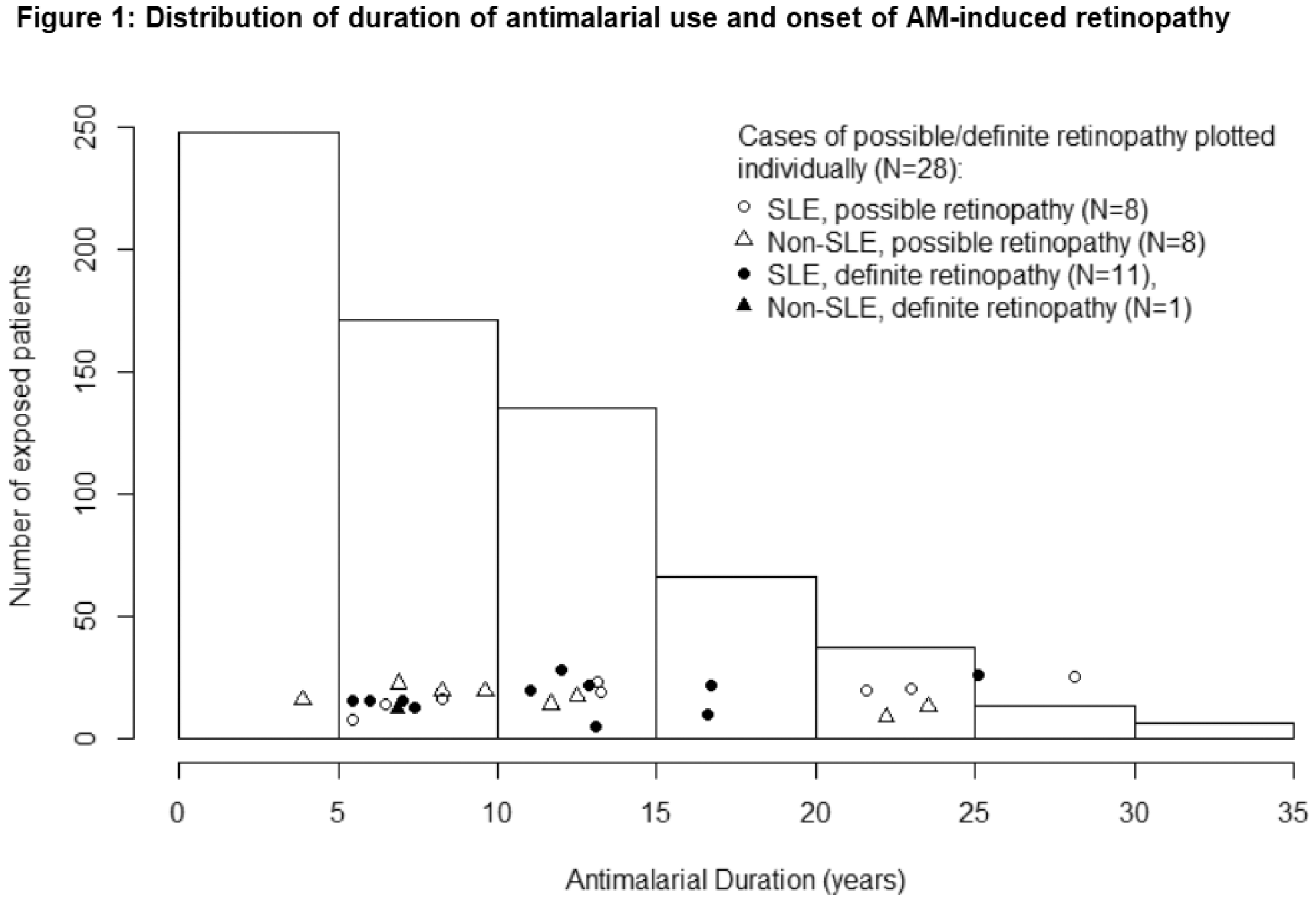
Objectives: To describe the pattern of AM-associated retinopathy, including diagnosis of SLE as a risk factor.
Methods: A chart review was conducted at an urban Canadian center. Each patient was classified as SLE, based on ACR criteria, or non-SLE. Minimum duration of AM use was 3 months. AM-induced retinopathy was classified as possible or definite, and was determined based on characteristic visual field loss, abnormal retinal imaging, and eye specialists’ opinion. Univariate and multivariate logistic regressions were performed to determine factors associated with definite AM-induced retinopathy. Sensitivity analyses included inclusion of possible AM-induced retinopathy and stratification of analysis by diagnosis and by CQ versus HCQ.
Results: Of the 680 patients, 282 patients had SLE and the remaining had RA (N=224), cutaneous lupus (N=41), or other connective tissue diseases (N=131). Patients with SLE tended to be younger, female, and had relatively more CQ and total AM exposure (
Patient characteristics. Data represented as N (%) or means (SD)
| SLE (N=282) | Non-SLE (N=398)* | Total (N=680) | P | |
|---|---|---|---|---|
| Age | 40.1 ± 15 | 51 ± 13.8 | 46.5 ± 15.3 | 5.72×10 -21 |
| Female | 258 (91%) | 333 (84%) | 591 (87%) | 4.19×10 -3 |
| AM duration (years) | 11.5 ± 8.1 | 7.3 ± 6.2 | 9.1 ± 7.3 | 3.52×10 -11 |
| CQ ever | 35 (12%) | 21 (5%) | 56 (8%) | 1.41×10 -3 |
*other connective tissue diseases and RA
In univariate logistic regression (
Univariate logistic regression for risk of AM-induced retinopathy. Data represented as N (%) or mean ± SD
| Definite retinopathy | Possible or definite retinopathy | |||||
|---|---|---|---|---|---|---|
| No retinopathy N=668 | Retinopathy
| P | No retinopathy N=652 | Retinopathy
| P | |
| Age | 46.5 ± 15.3 | 43.2 ± 14.3 | 0.452 | 46.4 ± 15.4 | 47.1 ± 12.4 | 0.832 |
| Female | 580 (87%) | 11 (92%) | 0.626 | 567 (87%) | 24 (86%) | 0.848 |
| Weight (kg) | 76.5 ± 19.5 | 67.3 ± 12.8 | 0.098 | 76.5 ± 19.5 | 73.5 ± 17.8 | 0.424 |
| SLE Diagnosis | 271 (41%) | 11 (92%) | 0.008 | 263 (40%) | 19 (68%) | 0.006 |
| AM duration (years) | 9 ± 7.4 | 11.7 ± 5.8 | 0.215 | 8.9 ± 7.3 | 12.8 ± 6.8 | 0.007 |
| AM> 5 years | 417 (63%) | 0 | - | 250 (40%) | 1 (3%) | 0.006 |
| HCQ dose (mg/kg/day) | 5.2 ± 15.5 | 5.9 ± 1.5 | 0.891 | 5.2 ± 15.6 | 5.3 ± 1.4 | 0.971 |
| HCQ total dose (g) | 1042 ± 913.8 | 1235 ± 1032 | 0.471 | 1340 ± 914 | 1187 ± 955 | 0.404 |
| CQ total dose (g) | 46 ± 205.1 | 225± 291 | 0.011 | 37.6 ± 174) | 318 ± 529 | 6.16×10 -7 |
| Renal Impairment | 100 (15%) | 2 (17%) | 0.883 | 99 (15%) | 3 (11%) | 0.506 |
| Hypertension | 298 (45%) | 5 (42%) | 0.832 | 285 (44%) | 18 (64%) | 0.038 |
| Diabetes | 61 (9%) | 1 (8%) | 0.924 | 59 (9%) | 3 (11%) | 0.765 |
Conclusion: The risk of AM-induced retinal toxicity increases after 5 years of use. SLE patients may be at increased risk due to longer treatment duration, AM choice, and underlying disease processes.
REFERENCES:
[1]Petri M, Elkhalifa M, Li J. 15 Frequency of hydroxychloroquine retinopathy in the hopkins lupus cohort. Lupus Science & Medicine 2019;6:doi: 10.1136/lupus-2019-lsm.15
Disclosure of Interests: Hsin Yen Liu: None declared, Gemma Cramarossa: None declared, Janet Pope Grant/research support from: AbbVie, Bristol-Myers Squibb, Eli Lilly & Company, Merck, Roche, Seattle Genetics, UCB, Consultant of: AbbVie, Actelion, Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Eicos Sciences, Eli Lilly & Company, Emerald, Gilead Sciences, Inc., Janssen, Merck, Novartis, Pfizer, Roche, Sandoz, Sanofi, UCB, Speakers bureau: UCB