fetching data ... 
Background: Limited joint mobility (LJM) is a musculoskeletal disorder caused by flexion contractures of hand is a common complication in systemic sclerosis (SSc) patients. The distal parts of the upper limb (hands and fingers) is the most involved site in SSc.
Objectives: In this study, we aimed to evaluate LJM in SSc patients and to determine the relationship between the clinical features of the disease.
Methods: A total of 113 patients (>18 years old) diagnosed with diffuse cutaneous systemic sclerosis (DcSSc) and limited cutaneous systemic sclerosis (LcSSc) and 104 healthy controls were included in this study. LJM was evaluated with “prayer sign” and “table top sign” tests. LJM staging was done by Rosenbloom classification method(1, 2). LJM (+) and LJM (-) patients were compared in terms of demographic findings (gender, age and duration of disease), laboratory results (ESR, CRP, ANA, anti-topoisomerase I and anti-centromere) and modified Rodnan Skin Score (mRSS) results.
Results: In our study, a total of 113 patients diagnosed with SSc and 104 healthy controls with similar age and gender distribution were included. While LJM (+) was detected in 75 (66.4%) (LcSSc = 38, DcSSc = 37) of the patients diagnosed with SSc, LJM (mild) (+) was detected in 3 (2.8%) of the control group. One of these people had right 2nd DIF joint contracture due to osteoarthritis, and 1 patient was found to have simple contractures due to minor hand injury previously (
Comparison of demographic findings between SSc and Control group
| SSc Group (n=113 ) | Control Group (n=104 ) | p value | |
|---|---|---|---|
| Age, year | 57.02 ± 11.58 | 58.47 ± 11.26 | 0.061 |
| Gender (F / M ) | 98 (86.7) / 15 (13.3) | 65 (62.5) / 39 (37.5) | 0.064 |
| CRP (mg/L ) | 5.45 ± 5.39 | 2.14 ± 1.12 | <0.001 |
| ESR (mm/hr ) | 25.19 ± 18.9 | 14.46 ± 10.09 | 0.024 |
| Smoking, n (% ) | |||
| Smoker | 89 (78.8) | 70 (67.3) | 0.464 |
| Non-Smoker | 24 (21.2) | 34 (32.7) | |
| LJM (Absent / Present ) | |||
| Present | 75 (66.4) | 3 (2.8) | <0.001 |
| Absent | 38 (33.6) | 101 (97.2) | |
| Rosenbloom classification | LcSSc (n=71) (% ) | DcSSc (n=42) (% ) | Total (n=113) (% ) |
| Normal | 46.5 | 11.9 | 33.6 |
| Mild | 22.5 | 14.3 | 19.5 |
| Moderate | 23.9 | 33.3 | 27.4 |
| Severe | 7.1 | 40.5 | 19.5 |
Comparison of demographic and clinical findings LJM(-) and LJM(+) in SSc
| LJM (-) (n=38 ) | LJM (+) (n=75 ) | p value | |
|---|---|---|---|
| Age, year | 54.16 ± 11.82 | 58.47 ± 11.26 | 0.061 |
| SSc Type | n (%) | n (%) | |
| LcSSc, n (%)
| 33 (56.8) | 38 (50.7) | <0.001 |
| 5 (13.2) | 37 (49.3) | ||
| Gender , F/M (% ) | 37 (97.3) / 1 (2.7) | 61 (81.3) / 14 (18.7) | 0.018 |
| Raynaud’s (symptom duration), month | 148 (44-456) | 150 (35-588) | 0.990 |
| Non-raynaud (symptom duration), month | 108 (28-458) | 138 (38-447) | 0.132 |
| mRSS, median | 2 (0-14) | 8 (0-36) | <0.001 |
| CRP (mg/L ) | 4.21 ± 4.48 | 6.08 ± 5.71 | 0.069 |
| ESR (mm/hr ) | 19.74 ± 10 | 27.95 ± 21.6 | 0.270 |
| Renal crisis, n (% ) | 1 (2.6) | 4 (5.3) | 0.662 |
| PAH, n (% ) | 8 (21.1) | 14 (18.7) | 0.762 |
| ANA positivity, n (% ) | 36 (94.7) | 70 (93.3) | 1 |
| Anti-centromere positivity, n (% ) | 18 (47.4) | 19 (25.3) | 0.01 |
| Anti-topoisomerase-1, n (% ) | 8 (21) | 34(45.3) | 0.01 |
| Smoking, n (% ) | n (%) | n (%) | |
| Non-smoker | 30(78.9) | 59 (78.7) | 0.970 |
| Smoker | 8 (21.1) | 16 (21.3) |
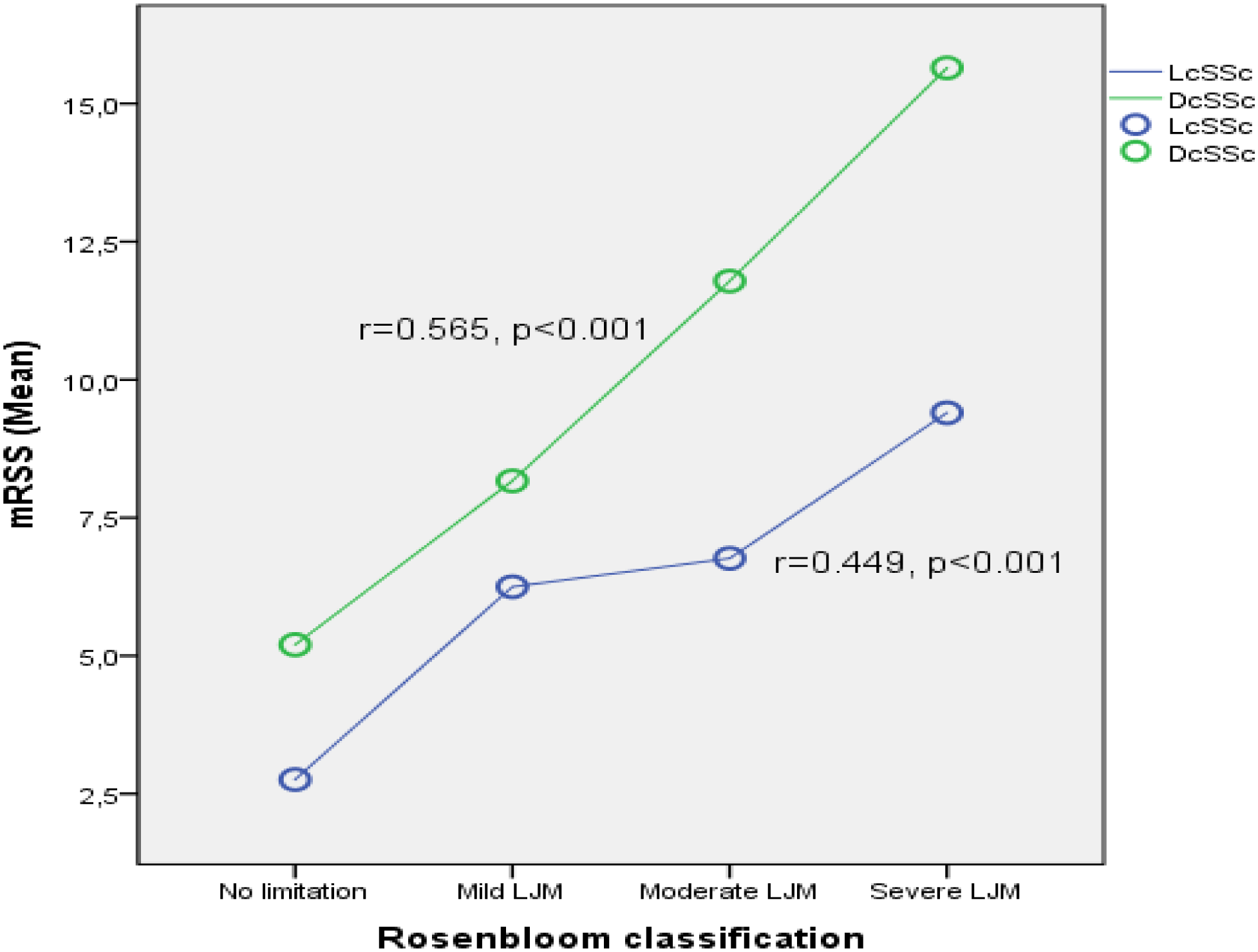
Conclusion: In our study, it was found that LJM staging positively correlated with mRSS and DcSSc patients had more severe LJM findings than LcSSc. We conclude that “prayer sign” and “table top sign” tests used in hand evaluation in SSc patients have similar clinical results with mRSS and can be easily performed in daily practice in about 3 minutes.
REFERENCES:
[1]Rosenbloom AL. Limitation of finger joint mobility in diabetes mellitus. The Journal of diabetic complications 1989; 3: 77-87.
[2]Nashel J, Steen V. Scleroderma mimics. Current rheumatology reports 2012; 14: 39-46.
Disclosure of Interests: None declared