fetching data ... 
Background: Infection is an important cause of mortality and morbidity in patients with systemic lupus erythematosus (SLE) and a common cause for hospitalization. Glucocorticoids (GC) may contribute to increased mortality.
Objectives: We performed a 10-year retrospective study of SLE patients hospitalized for infection, and the clinical predictors of mortality, especially GC dose, in these patients.
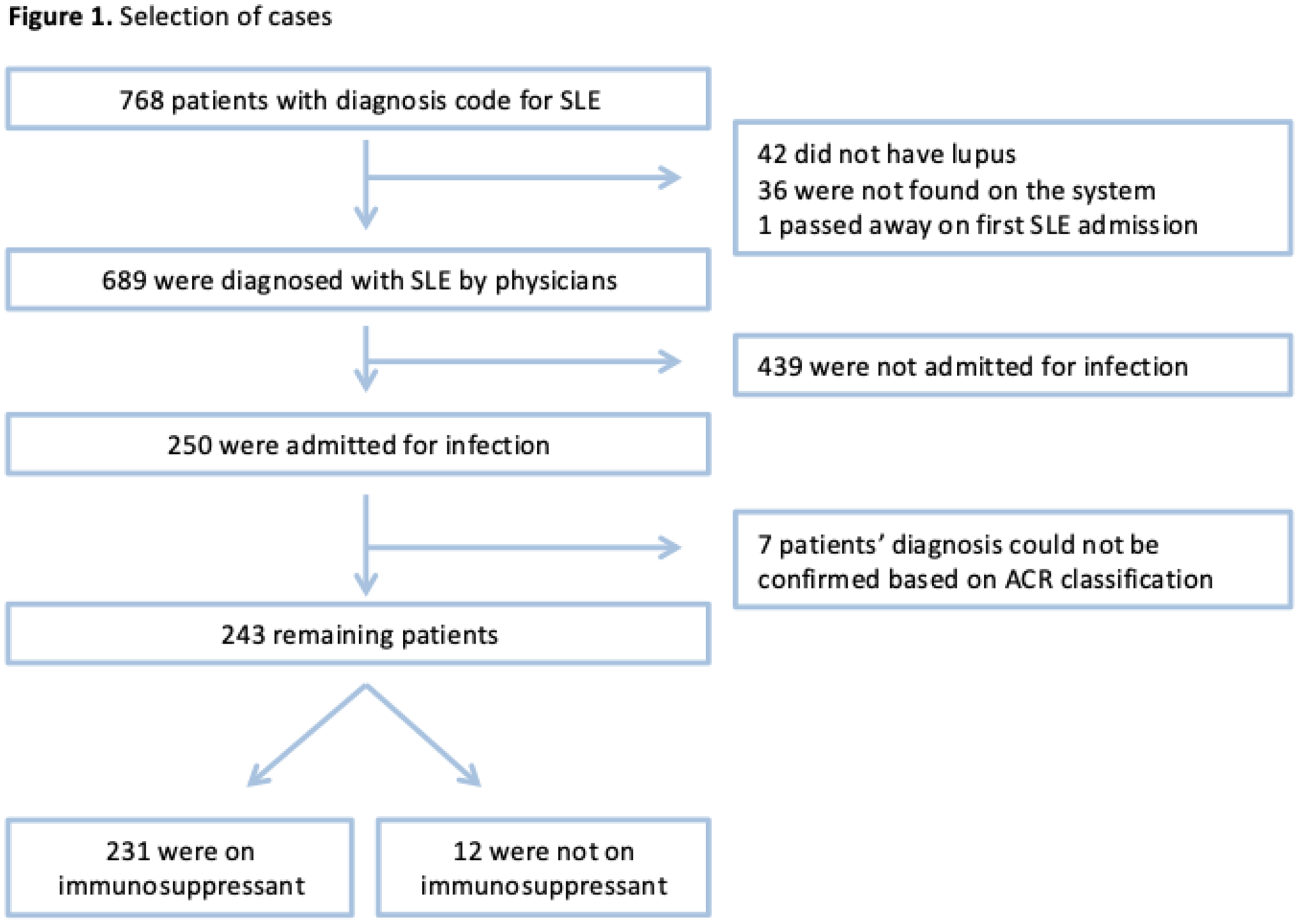
Methods: Diagnosis codes for SLE were obtained from the electronic medical records for hospitalized patients from 2005 to 2015. Chart review was performed to ascertain the indication for hospitalization. The first hospitalization for infection (if any) was used as the index admission. Demographic and clinical characteristics, infection site and immunosuppressive drugs over the past month were abstracted. Multivariable logistic regression was used to determine predictors of all-cause mortality at 1 year.
Results: Diagnosis codes were obtained for 768 unique SLE patients with 3660 hospitalization episodes over 10 years, of which 689 had a physician diagnosis of SLE on chart review. Of these, 250 (36%) had an index admission for infection. 243/250 (97.2%) fulfilled the ACR 1997 criteria for SLE and were studied further (
Predictors of mortality
| Factors | Univariable
| P-value | Multivariable
| P-value |
|---|---|---|---|---|
| Age at admission (years) | 1.04 (1.005, 1.07) | 0.02 | 1.07 (1.02,1.12 ) | 0.005 |
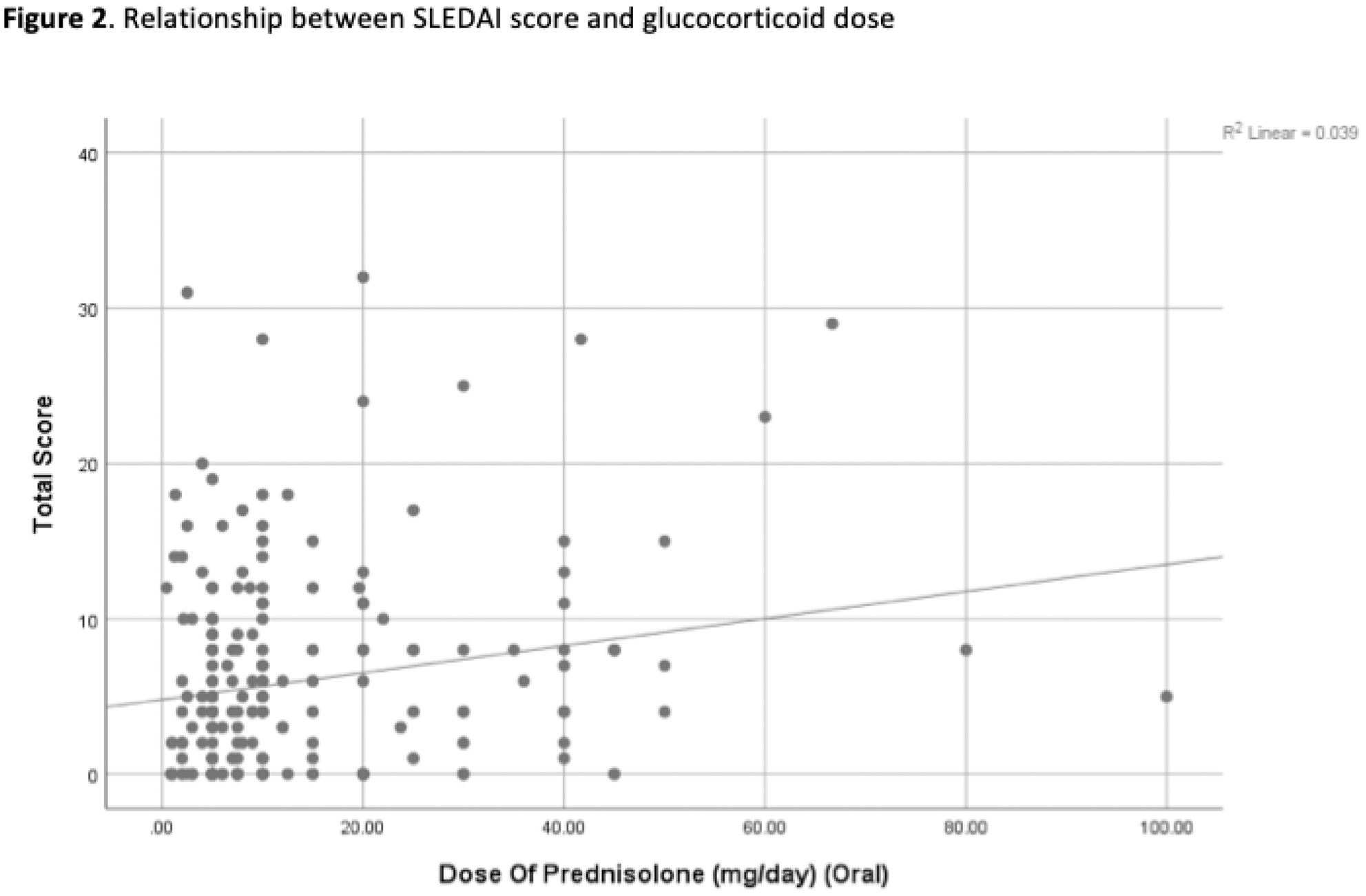
| Average dose of oral prednisolone (mg/day) | 1.04 (1.01, 1.06) | 0.006 | 1.05 (1.02,1.09 ) | 0.002 |
| Gender (female vs male) | 3.52 (1.22, 10.12) | 0.02 | 0.37 (0.07, 2.10) | 0.26 |
| Disease duration > 10 years | 1.27 (0.49, 3.33) | 0.62 | ||
| Positive blood culture | 0.54 (0.17, 1.75) | 0.30 | ||
| Site of infection
| 1 (reference) | 0.17 | 0.06 | |
| Respiratory | 1.09 (0.28, 4.29) | 0.90 | 0.71 (0.09, 5.57) | 0.74 |
| Renal | 0.27 (0.03, 2.48) | 0.25 | 0.44 (0.03, 5.94) | 0.54 |
| Skin, Gynecological, Other | 0.94 (0.25, 3.51) | 0.93 | 1.04 (0.16, 6.74) | 0.96 |
| Bone | 11.75 (1.29, 107.1) | 0.03 | 42.24 (2.76, 646.8 ) | 0.007 |
| Primary Bacteremia | 0.00 (0.00, 0.00) | 0.99 | 0.00 (0.00, 0.00) | 0.99 |
| SLEDAI score ≥4 | 1.23 (0.47, 3.21) | 0.66 | 0.65 (0.15, 2.74) | 0.56 |
| Diabetes Mellitus | 0.46 (0.14, 1.50) | 0.20 | 1.61 (0.31, 8.3) | 0.57 |
| Chronic Kidney Disease | 0.30 (0.11, 0.78) | 0.01 | 4.78 (1.06, 21.54 ) | 0.04 |
| Cancer | 0.18 (0.04, 0.77) | 0.02 | 3.52 (0.25, 48.82) | 0.35 |
Conclusion: Higher dose of oral GC was an independent predictor of mortality, even after adjusting for disease activity. It is important to prescribe the minimum effective dose of GC in SLE patients with infection, especially in older patients with CKD and bone infection.
Disclosure of Interests: Thurston Yan Jia Heng: None declared, Nicholas Chew: None declared, Kexin Amanda Choo: None declared, Aisha Lateef: None declared, Manjari Lahiri Grant/research support from: Manjari Lahiri is the site principal investigator for the Singapore National Biologics Register, which is a multi-pharmaceutical funded register, in which industry sponsors provide support through the Chapter of Rheumatologists, Singapore. Dr Lahiri does not personally receive any remuneration.