fetching data ... 
Background: Takayasu Arteritis is a chronic, large vessel arteritis that commonly involves the aorta and its major branches, mostly the ascending/descending aorta, subclavian arteries, and carotids [1].
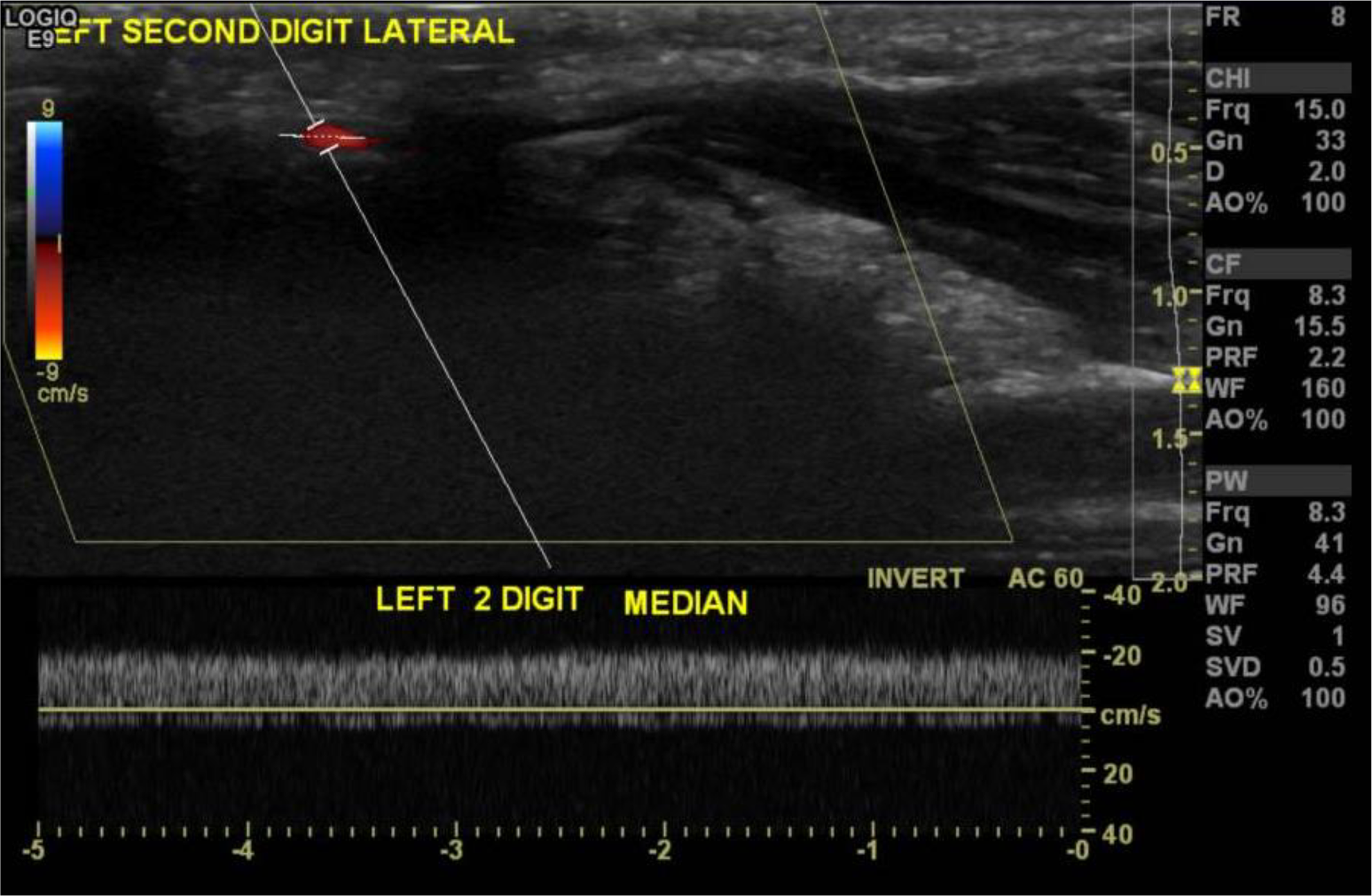
Herein, we report a case of a 23 year-old medically free Indian male who presented to our hospital in acute distress complaining of cough, hemoptysis and shortness of breath for one week as well as intermittent fever and fatigue for five months. He presented with a BP of 140/100 mmHg as well was both systolic and early diastolic murmurs in the mitral and aortic areas, respectively. He also had a paraumbilical bruit and unilateral clubbing in the left hand with digital ischemia of the left index finger. Doppler ultrasound of the left arm showed monophasic flow pattern with low velocity in left distal radial, distal ulnar, and all digital arteries, except the second digital arteries; low velocity in the median artery; and no flow in the lateral artery of second digit (
Unilateral clubbing in patients with TA occurs as a result of subclavian artery stenosis that leads to tissue ischemia and hypoxia [2-4]. In turn, the bone marrow release megakaryocytes, which enter the systemic circulation when an A-V shunt exists [5]. Platelet-derived growth factor (PDGF) (release from megakaryocytes) and vascular endothelial growth factor (VEGF) levels are highly expressed in the connective tissues of nail beds, leading to its proliferation and platelets clumps‘ accumulation [6, 7].
Objectives: To report the fourth case worldwide and third case of an adult, respectively, with Takayasu’s arteritis who presents with unilateral clubbing.
Methods: Our patient was started on pulse steroid therapy of methylprednisolone 1 gram IV od for 5 days and later switched to prednisolone 20 mg po BID. He also received methotrexate 10 mg PO once weekly and rituximab 750 mg IV stat; another dose of rituximab was given two weeks later.
Results: His clubbing has significantly improved within 2 weeks of starting immunosuppressive therapy. He was discharged with follow up on methotrexate 12.5 mg PO once weekly and prednisilone 20 mg PO OD (to be tapered). Clubbing improved by a rate of 60% two weeks following discharge in two weeks.
Conclusion: In all four cases of Takayasu arteries presenting with unilateral clubbing, patients’ clinical condition including presence of clubbing improved after initiation of immunosuppressive therapy.
REFERENCES:
[1]Alibaz-Öner, F., Aydin, S. Z., & Direskeneli, H. (2015). Recent advances in Takayasu’s arteritis. European Journal of Rheumatology , 2 (1), 24–30.
[2]Kaditis AG, Nelson AM, Driscoll DJ. Takayasu\’s arteritis presenting with unilateral digital clubbing. J Rheumatol 1995;22:2346-8.
[3]Ishikawa M, Okada J, Kondo H. Takayasu’s arteritis with transient clubbed finger. Clin Exp Rheumatol 1999;17:629-30.
[4]Bivilibal M, Duru N, Dogdu G, Elevli M, Ayta S. A Takayasu’s Arteritis Case with Unilateral Digital Clubbing. Turk J Rheumatol. 2011;26(2):163–166.
[5]Martínez-Lavín M. Hypertrophic osteoarthropathy. Curr Opin Rheumatol. 1997 Jan;9(1):83-6. Review. PubMed PMID: 9110140.
[6]Dickinson CJ, Martin JF. Megakaryocytes and platelet clumps as the cause of finger clubbing. Lancet 1987;2:1434-5.
[7]Atkinson S, Fox SB. Vascular endothelial growth factor (VEGF)-A and platelet-derived growth factor (PDGF) play a central role in the pathogenesis of digital clubbing. J Pathol 2004;203:721-8.
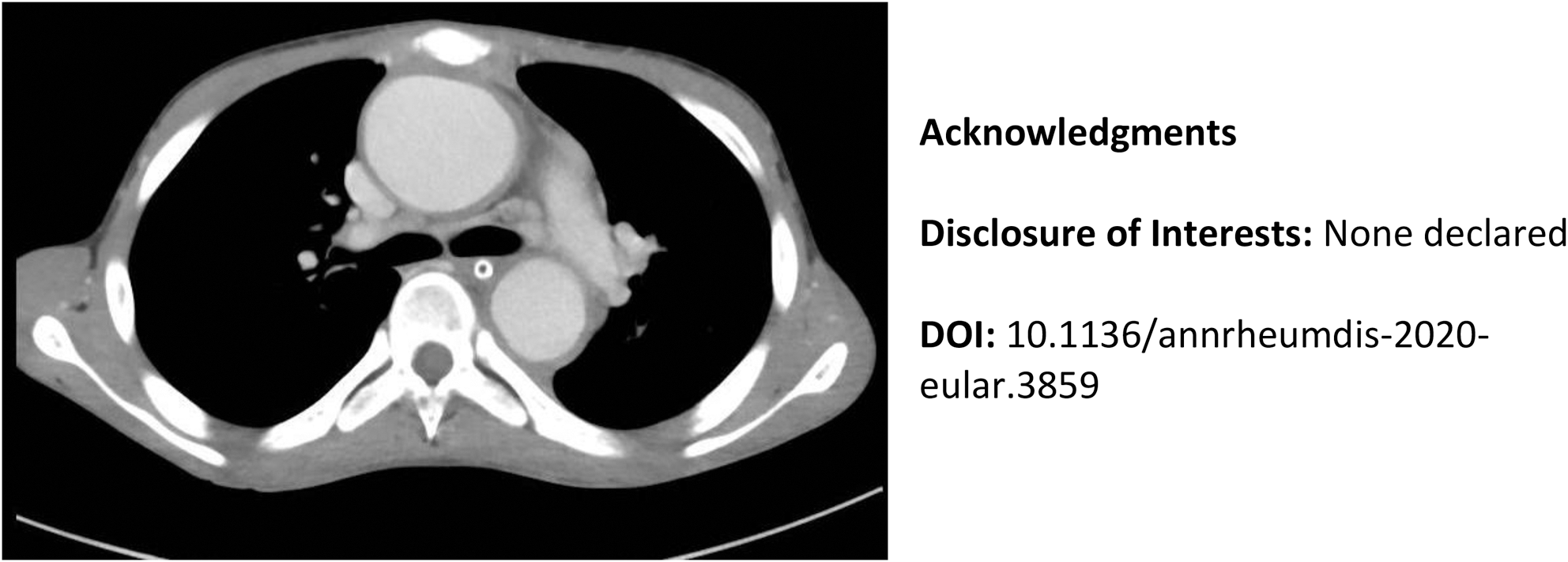
Disclosure of Interests: None declared