fetching data ... 
Background: Anti-Ku antibodies have been associated with various connective tissue diseases, including myositis, arthritis, interstitial lung disease and glomerulonephritis 1 .
Objectives: We present a case of a woman initially diagnosed with biopsy proven Kikuchi-Fujimoto disease who later developed a rapidly progressive myositis in association with anti-Ku antibodies.
Methods: A 47 year-old woman, originally from Myanmar, presented with lymphadenopathy, myalgia, fatigue, livedo reticularis and low-grade fever for the previous 6 months. This was initially diagnosed as a viral infection. Her myalgia progressed with proximal muscle weakness in both legs and associated rise in creatine kinase levels to 349U/L (normal range 25-200). She also developed dyspnoea, an erythematous rash, mouth ulcers and unintentional weight loss.
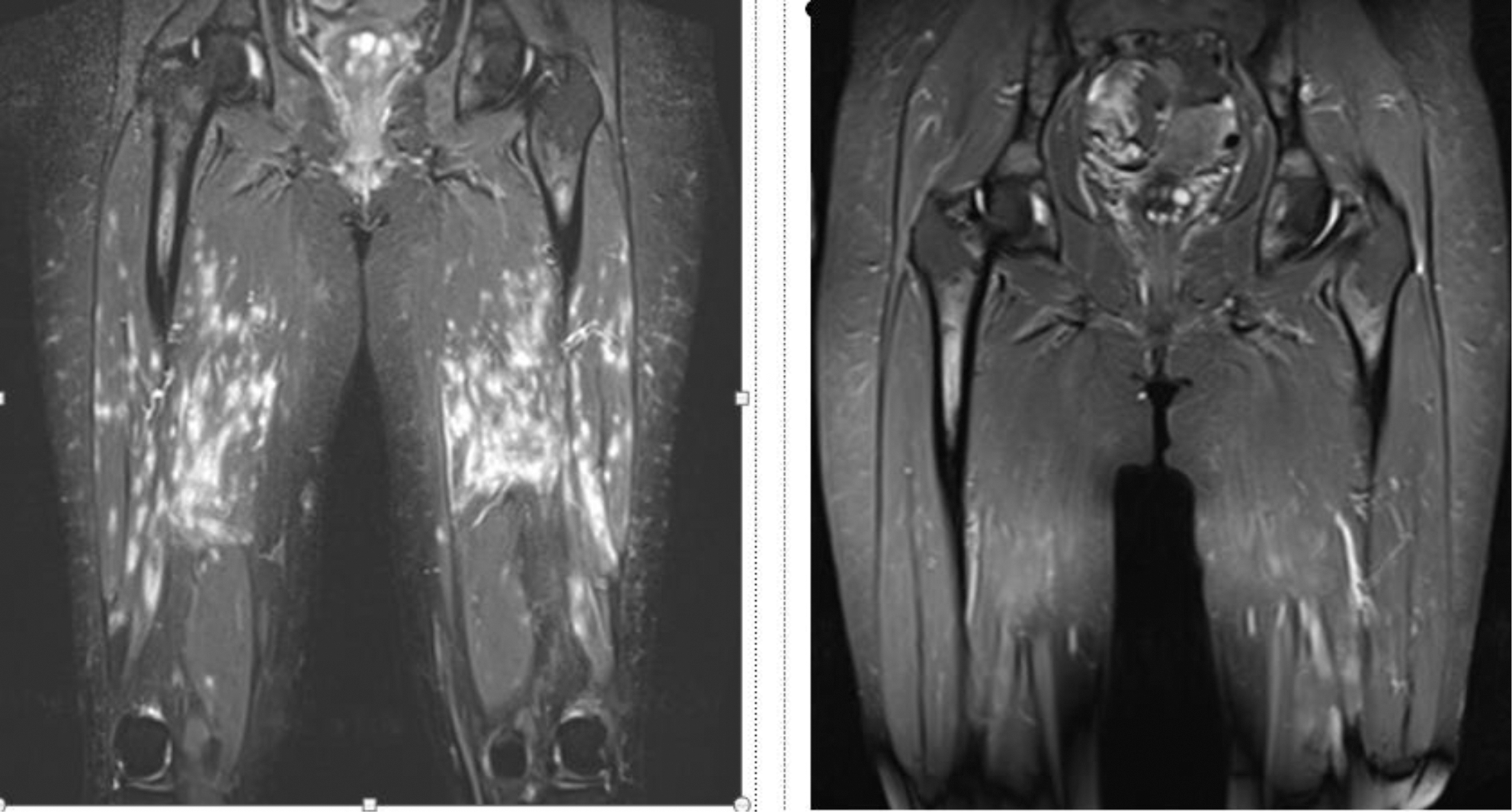
Blood tests show a lymphopenia and progressively rising CK, with a maximum level of 516 U/L. MRI whole body confirmed a widespread diffuse myositis in her upper and lower limbs, with an unusual ‘speckled’ pattern. High resolution CT Chest was normal. C3 0.40 g/l (normal range 0.75-1.65) and C4 0.12 g/l (0.14-0.54) were low, with a positive ANA (1:160) and Ro-60 antibody. dsDNA, antiphospholipid screen and virology screens were all negative. Extended myositis panel revealed positive anti-Ku antibodies. Axillary lymph node biopsy confirmed necrotising lymphadenitis, consistent with Kikuchi-Fujimoto disease.
Results: She was initially treated with low dose Prednisolone and Hydroxychloroquine, with a limited response. Due to progressive myositis, pulsed IV Methylprednisolone 1g was provided over 3 days and mycophenolate mofetil (MMF) was started.
An inpatient stay was needed after developing an axillary node abscess and a chest infection. This was treated with intravenous antibiotics and repeated aspirations. Due to progressive myositis on a background of sepsis, intravenous immunoglobulin (IVIG) was administered over 5 days. Our patient made a good recovery, with normalization of CK levels and resolution of the myositis noted on repeat MRI scan. She remains on MMF as maintenance therapy.
Conclusion: Anti Ku antibodies appear to be associated with 2 spectrums of disease – elevated CK levels with interstitial lung disease and renal disease associated with anti-dsDNA antibodies 1 To our knowledge this is the first report in association with Kikuchi-Fujimoto disease. The combination of MMF and IVIG appears to have been effective treatment and her renal function remains stable, although we are monitoring the patient carefully for the possible development of interstitial lung disease.
REFERENCES:
[1]Spielmann L, Nespola B, Séverac F, et al. Anti-Ku syndrome with elevated CK and anti-Ku syndrome with anti-dsDNA are two distinct entities with different outcomes. Annals of the Rheumatic Diseases 2019;78:1101-1106.
Disclosure of Interests: None declared