fetching data ... 
Background: Cystoid Macular Edema (CME) is the most important cause of blindness in non-infectious uveitis (NIU) (1). Corticosteroids and conventional and/or biological immunosuppressant may be required (1-6). High-dose intravenous methylprednisolone (IVMP) pulse therapy may induce a rapid improvement.
Objectives: To evaluate the efficacy and safety of IVMP pulse therapy in CME of different immune mediated inflammatory diseases (IMID).
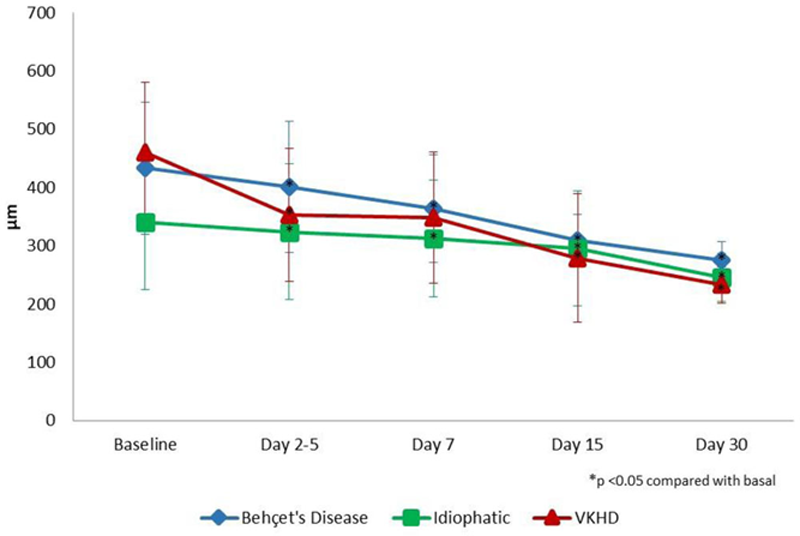
Methods: Multicentre study of 66 patients with severe ocular inflammation who received IVMP. The underlying diseases were: Vogt Koyanagy Harada disease (VKHD)(n=24), Behçet’s disease (BD) (19) and idiopathic NIU (23). The main outcome variable was macular thickness and macular edema (Optical coherence tomography [OCT] >300 μm); that was assessed at 0 (basal), 2-5, 7, 15 and 30 days after IVMP.
The results are expressed as mean ±SD for normally distributed variables, or as median [IQR] when are not. Comparison of continuous variables was performed using the Wilcoxon test.
Results: We studied 43♀/ 23♂ patients. The main features are shown in
Main features of 66 patients with cystoid macular edema.
|
VKHD
|
Idiophatic
|
Behcet’s disease
|
Overall
|
|
| Men/Women, n | 5/19 | 9/14 | 9/10 | 66 |
| Mean age (years ) | 42 ± 11 | 47 ± 15 | 33 ± 10 | - |
| Unilateral/Bilateral, n (% ) | 2 (8.3) /22 (91.7 ) | 10 (43.5) /13 (56.5) | 4 (21) /15 (79) | 16/50 |
| Inflammatory ocular patterns, n (% ) | ||||
| Posterior uveitis | 6 (25) | 9 (39.1) | 3 (15.8) | 18 |
| Panuveitis | 18 (75) | 14 (60.9) | 16 (84.2) | 48 |
| Laboratory data, n (% ) | ||||
| ANA | 2 (8.34) | 2 (8.7) | 0 (0) | 4 |
| HLA B27 | 0 (0) | 4 (17.4) | 0 (0) | 4 |
| HLA B29 | 0 (0) | 1 (4.3) | 0 (0) | 1 |
| HLA B51 | 0 (0) | 5 (21.7) | 8 (42) | 13 |
A rapid and maintained statistically improvement was observed in OCT values in all underlying diseases (
Conclusion: High-dose IVMP pulse therapy is useful and safe in the prompt control of CME, regardless of the underlying IMID.
REFERENCES:
[1]Vegas-Revenga N, et al. Am J Ophthalmol. 2019; 200:85-94. doi: 10.1016/j.ajo.2018.12.019.
[2]Calvo-Río V, et al. Clin Exp Rheumatol. 2014;32(4 Suppl 84): S54-7. PMID: 25005576.
[3]Santos-Gómez M, et al. Clin Exp Rheumatol. 2016;34(6 Suppl 102): S34-S40. PMID:27054359.
[4]Atienza-Mateo B, et al. Rheumatology (Oxford) 2018;57(5):856-864. doi: 10.1093/rheumatology/kex480.
[5]Atienza-Mateo B, et al. Arthritis Rheumatol. 2019; 71(12):2081-2089. doi: 10.1002/art.41026.
[6]Martín-Varillas JL, et al. Ophthalmology. 2018;125(9):1444-1451. doi: 10.1016/j.ophtha.2018.02.020.
Improvement of OCT in 66 patients with cystoid macular edema.
Disclosure of Interests: None declared