fetching data ... 
Background: Therapeutic decisions in RA patients should be based on regular disease activity assessment using scores like the Simplified Disease Activity Index (SDAI) or the Clinical Disease Activity Index (CDAI) [1]. The CDAI has the benefit of being immediately available, while the SDAI encompasses with the C-reactive protein (CRP) an acute phase reactant and therefore is the recommended score for the use in clinical trials. However, CRP determination takes hours to days, thus hindering the treat-to-target concept using the SDAI. Quick quantitative CRP (qCRP) tests allow CRP measurement within a few minutes. Therefore, qCRP based SDAI (SDAI-Q) could combine the advantages of both scores.
Objectives: To validate the SDAI-Q in a prospective, multicenter study of RA patients.
Methods: The study was conducted in five centers in Berlin, Germany. Consecutive adult (≥ 18 years) RA patients were included. In addition to a rheumatological assessment, including patient reported outcomes, routine CRP was measured in the local labs. Additionally, a qCRP testing with the „QuikRead go instrument“ (Aidian Oy, Finland) was performed locally (measurement range 0.5 - 200 mg/l). Statistical analysis included descriptive statistics, cross tabulation and weighted Cohen´s kappa comparing disease activity categories, Bland-Altman plots and intraclass correlation coefficient (ICC) for CRP, qCRP, SDAI, SDAI-Q and CDAI.
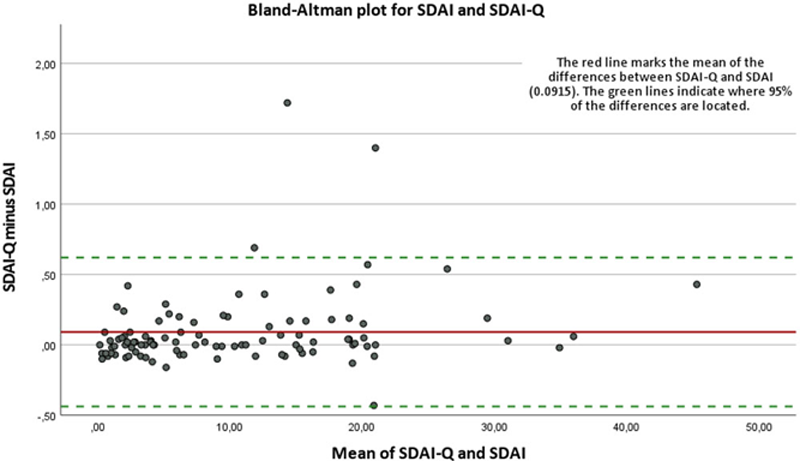
Results: In this study 100 RA patients were included (mean age: 60.9 years, mean disease duration: 11.4 years, 73.0% were female, 63.0% RF positive, 57.0% ACPA positive, 49.0% positive and 29% negative for both parameters). 75.0% were treated with csDMARD, 15% with tsDMARDs, 39.0% with bDMARDs and 40% with glucocorticoids (mean prednisolone equivalent: 5.4 mg prednisolone/d). Mean CRP and qCRP-levels were 6.97 and 7.89 mg/l, respectively (ICC 0.992; 95%CI: 0.987; 0.995). Comparing SDAI-Q and SDAI, all patients (100%) achieved the same disease activity status (
Conclusion: SDAI-Q showed an absolute agreement with SDAI on the assignment to disease activity categories with the important advantage of time. With SDAI-Q, rheumatologists could base their clinical decision-making immediately on an index-based disease activity measurement by using a composite score considering acute phase reactants. Consequently, SDAI-Q can be integrated in clinical routine and clinical trials and could be implemented into the treat-to-target concept in RA patients.
REFERENCES:
[1]Smolen JS, et al. Ann Rheum Dis. 2016 Jan; 75(1):3-15.
A) Disease activity categories by SDAI-Q vs. SDAI; B) Disease activity categories by SDAI-Q vs. CDAI
| A | SDAI-Q (n = 100 ) | ||||
| Remission (≤ 3.3) | Low Disease Activity (> 3.3 and ≤ 11) | Moderate Disease Activity (> 11 and ≤ 26) | High Disease Activity (> 26) | ||
| SDAI | Remission (≤ 3.3) | 28 (28.0% ) | |||
| Low Disease Activity (> 3.3 and ≤ 11) | 31 (31.0% ) | ||||
| Moderate Disease Activity (> 11 and ≤ 26) | 35 (35.0% ) | ||||
| High Disease Activity (> 26) | 6 (6.0% ) | ||||
| B | SDAI-Q (n = 100 ) | ||||
| Remission (≤ 3.3) | Low Disease Activity (> 3.3 and ≤ 11) | Moderate Disease Activity (> 11 and ≤ 26) | High Disease Activity (> 26) | ||
| CDAI | Remission (≤ 2.8) | 26 (26.0% ) | |||
| Low Disease Activity (> 2.8 and ≤ 10) | 2 (2.0% ) | 28 (28.0% ) | 2 (2.0% ) | ||
| Moderate Disease Activity (> 10 and ≤ 22) | 3 (3.0% ) | 33 (33.0% ) | |||
| High Disease Activity (> 22) | 6 (6.0% ) | ||||
Fields highlighted in red indicate that disease activity categories do not match.
SDAI = Simplified Disease Activity Index;
SDAI-Q = SDAI calculated with a quick quantitative CRP assay;
CDAI = Clinical Disease Activity Index.
Bland-Altman plot for SDAI and SDAI-Q Acknowledgements
The authors would like to deeply thank Braun T, Doerwald C, Deter N, Höppner C, Lackinger J, Lorenz C, Lunkwitz K, Mandt B, Sron S and Zernicke J for their practical support and coordinating the study.
Funding statement:
The AQUA study was supported by an unrestricted research grant from Novartis. Testing kits were provided free of charge from Aidian Oy, Finland.
Disclosure of Interests: None declared