fetching data ... 
Background: Hydroxychloroquine (HCQ) is a widely used drug especially in connective tissue disorders such as Systemic Lupus Erythematosus (SLE). Cardiac adverse effects of long-term use of HCQ remains controversial.
Objectives: To assess cardiac adverse effects of long-term use of HCQ in SLE.
Methods: Observational single center study of 109 patients with SLE treated with HCQ for more than 3 months. The main outcomes were cardiac structural and conduction disorders in a 12-lead electrocardiogram and/or echocardiogram at baseline and during HCQ treatment.
Results: We studied 109 patients (95 women/14 men; mean age 66.9±14.7 years). Main cardiovascular history was hypertension (n=61, 56.0%), diabetes mellitus (n=16, 14.7%) and renal impairment (n=11, 10.1%). HCQ was used for 11.7±8.9 years. Initial median SLE Disease Activity Index 2000 (SLEDAI-2K) was 7 [3.75-11]. At baseline, 27 (24.8%) patients had conduction disorders and 15 (13.7%) had structural abnormalities: Most prevalent cardiac alterations were Left Anterior Fascicular Block (LAFB) (n=9, 8.3%), left ventricular hypertrophy (n=9, 8.3%) and right bundle branch block (n=8, 7.3%). After 11.7±8.9 years of follow-up (mean HCQ cumulative dose: 1042.2±267.5 g; median SLEDAI-2K 1 [0-4]), there was a significant increase in conductions disorders (n=41, 37.6%, p=0.011) and in LAFB (n=16, 14.7%, p=0.021). There was no statistically significant increase in structural abnormalities (n=21, 19.7%, p=0.629).
Main cardiac abnormalities at baseline and after 11.7±8.9 years of follow-up are summarized in
Main cardiac abnormalities at baseline and after follow-up.
| Baseline | After follow-up | p | |
| Conduction disorders, n (%) | 27 (24.8) | 41 (37.6) | 0.011 |
| Left anterior fascicular block | 9 (8.3) | 16 (14.7) | 0.021 |
| Right bundle branch block | 7 (6.4) | 8 (7.3) | 1.0 |
| Atrioventricular block | 4 (3.6) | 11 (10.1) | 0.092 |
| Incomplete right bundle branch block | 4 (3.6) | 5 (4.6) | 1.0 |
| Short PR interval | 2 (1.8) | 4 (3.7) | 0.5 |
| Prolonged QT corrected interval | 2 (1.8) | 4 (3.7) | 0.625 |
| Left bundle branch block | 1 (0.9) | 5 (4.6) | 0.125 |
| Atrial Fibrillation | 1 (0.9) | 5 (4.6) | 0.219 |
| Structural abnormalities, n (%) | 15 (13.7) | 21 (19.7) | 0.629 |
| Ventricular hypertrophy | 9 (8.3) | 9 (8.3) | 1.0 |
| Atrial enlargement | 6 (5.5) | 13 (11.9) | 0.096 |
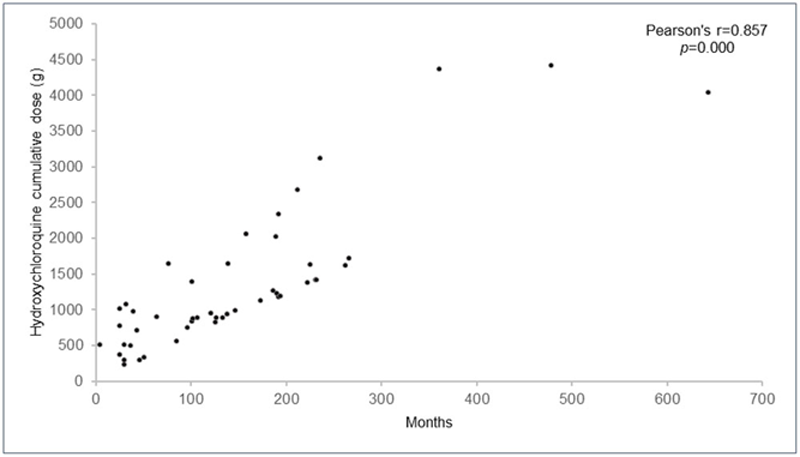
Time of occurrence of cardiac adverse effect in relation to hydroxychloroquine cumulative dose.
Conclusion: Conduction disorders were more prevalent than structural abnormalities. Patients with SLE treated with HCQ had a significant increase in LAFB. Use of electrocardiogram and/or echocardiogram may be helpful in monitoring cardiac adverse effects.
Disclosure of Interests: Alba Herrero-Morant: None declared, Adrián Margarida-de Castro: None declared, Raquel Pérez-Barquín: None declared, Jon Zubiaur-Zamacola: None declared, Miguel Á. González-Gay Speakers bureau: AbbVie, Pfizer, Roche, Sanofi, Lilly, Celgene and MSD, Grant/research support from: AbbVie, MSD, Jansen and Roche, Ricardo Blanco Speakers bureau: AbbVie, Pfizer, Roche, Bristol-Myers, Janssen, Sanofi, Lilly and MSD, Grant/research support from: AbbVie, MSD, and Roche