fetching data ... 
Background: There is an increase over time in studies adopting cluster analysis (CA) to identify causes, patterns and severity in rheumatic diseases. 1 However, CA has not been used to identify patterns of causes-of-death in patients with systemic lupus erythematosus (SLE).
Objectives: 1) to identify homogeneous groups of patients according to their causes-of-death, 2) to identify homogeneous groups of cause-of-death combinations and 3) to determine the potential prognostic value of the identified patterns.
Methods: This is a population-based study using the mortality register of Villa Clara (province of Cuba) between 1990 and 2019. Based on International Classification of Disease (ICD), Nine and Tenth Revision (ICD-9, code 710.0 and ICD-10, code M32), there were identified the SLE-related deaths (any mention on the death certificate) and their associated causes-of-death. Two hierarchical CA with Ward’s method was carried out, based on the associated causes-of-death: one to conglomerate patients and another one to conglomerate variables. To identify differences in socio-demographic characteristics and causes-of-death between each cluster, Chi-square test, Fisher’s exact test and Kruskal-Wallis test were used as appropriate. Multivariate Poisson regression model corrected for over-dispersion was used to determine the prognostic value of the clusters. Years of potentially life lost (YPLL) was defined as a dependent variable. To calculate YPLL, each decedent’s age at death was subtracted from a predetermined age of 75 years.
Results: A total of 141 patients were analyzed, which were grouped into three clusters. The socio-demographic features and causes-of-death that characterized each cluster are summarized in
Socio-demographic characteristics and top ten causes-of-death according to clusters.
| Variable |
Cluster 1
|
Cluster 2
|
Cluster 3
| P value |
| Age at death median (IR) | 36(28.5 to 50.2) | 46(30.0 to 56.0) | 49(39.0 to 63.2) | 0.022 |
| Sex n(%) | ||||
| Male | 4(28.6) | 8(57.1) | 2(14.3) | 0.873 |
| Female | 36(28.3) | 63(49.6) | 28(22.0) | |
| Skin color n(%) | ||||
| White | 18(21.4) | 45(53.6) | 21(25.0) | 0.070 |
| Non White | 22(38.6) | 26(45.6) | 9(15.8) | |
| Associated causes-of-death n(%) | ||||
| Acute respiratory failure | 2(11.8) | 6(35.3) | 9(52.9) | 0.006 |
| Chronic kidney disease | 31(96.9) | 0(0) | 1(3.1) | 0.000 |
| Essential hypertension | 2(22.2) | 6(66.7) | 1(11.1) | 0.734 |
| Heart failure | 3(25.0) | 9(75.0) | 0(0) | 0.093 |
| Lupus nephritis | 39(95.1) | 2(4.9) | 0(0) | 0.000 |
| Multiple organ failure | 2(18.2) | 5(45.5) | 4(36.4) | 0.496 |
| Pericarditis | 4(40.0) | 5(50.0) | 1(10.0) | 0.569 |
| Pneumonia | 5(14.7) | 6(17.6) | 23(67.6) | 0.000 |
| Pulmonary embolism | 4(20.0) | 15(75.0) | 1(5.0) | 0.043 |
| Septicemia | 4(22.2) | 0(0) | 14(77.8) | 0.000 |
YPLL: Years of potentially life lost. IR: interquartile rank.
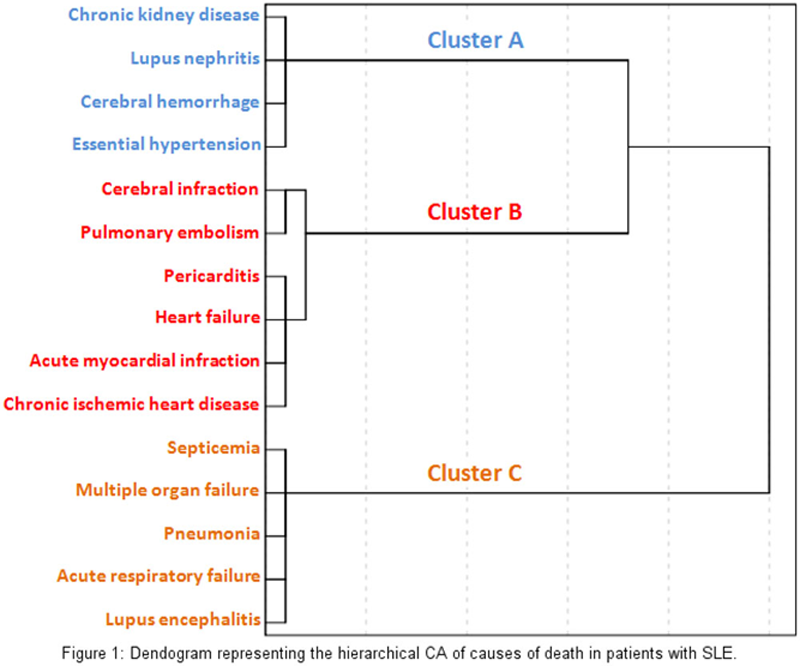
Conclusion: Three clusters of patients were identified, the one with higher prevalence of causes-of-death expressing renal damage presented higher mortality burden. The patterns of causes-of-death were mainly shaped by renal, cardiovascular and infectious causes. Better understanding of the association among causes of death, improves our comprehension of SLE and facilitate its clinical management.
REFERENCES:
[1]Han L, Benseler SM, Tyrrell PN. Cluster and Multiple Correspondence Analyses in Rheumatology. Rheum Dis Clin N Am. 2018; 44:349-60.
Disclosure of Interests: None declared