fetching data ... 
Background: Idiopathic Inflammatory Myopathies (IIMs) patients are at risk of bone mineral density (BMD) loss due to systemic inflammation, use of glucocorticoids (GCs) and disability. Cross sectional study showed 70% of IIMs patients had reduced BMD but whether they were at excessive risk compared to controls were unknown.
Objectives: To compare the prevalence of reduced BMD between IIMs patients, non-rheumatological controls, rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) patients and to determine the clinical determinants of BMD in IIMs patients.
Methods: This was a single centre retrospective case control study. BMD at lumbar spine L1-L4 and neck of femur (NOF) were assessed by dual-energy X-ray absorptiometry (DXA) scans. The prevalence of reduced BMD and osteoporosis in Chinese IIMs patients and age-and-sex-matched non-rheumatological controls were compared. The BMD of female IIMs were then compared to age matched female RA and SLE patients in the secondary analysis. Binary logistic regression was used for adjustment of confounders. The demographics and clinical variables independently associated with BMD were determined by linear regression.
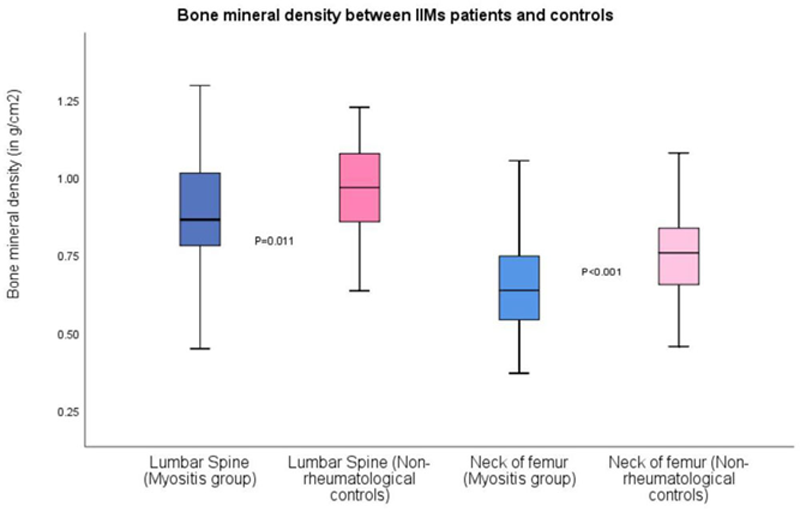
Results: A total of 230 patients were recruited including 65 IIMs, 65 non-rheumatological controls, 50 RA and 50 SLE patients. The mean age was 58.6±10.96 years and 76.9% were female. There was no significant difference on demographics between the two groups. Almost all IIMs patients (98%) and 52% of controls had exposed to GCs (p<0.001). Significantly more IIMs patients had used immunosuppressants (92.3% vs 38.5%, p<0.001) and biologics (13.8% vs 1.5%, p=0.01). The prevalence of reduced BMD and osteoporosis were significantly higher in IIMs patients than non-rheumatological control (Reduced BMD: 73.8% vs 43.1%, p=0.043; Osteoporosis: 29.2% vs 13.8%, p=0.033) (
Conclusion: Reduced BMD was more prevalent in IIM patients than non-rheumatological controls. Lower BMI and more advanced age were associated with lower BMD. Vigilant monitoring of BMD and use of antiresorptive treatment should be considered in IIM patients.
REFERENCES:
[1]Briot K, Geusens P, Em Bultink I et al. Inflammatory diseases and bone fragility. Osteoporos Int. 2017;28:3301-14.
[2]So H, Yip ML, Wong AKM. Prevalence and associated factors of reduced bone mineral density in patients with idiopathic inflammatory myopathies. Int J Rheum Dis. 2016;19:521-8.
Prevalence of reduced BMD in IIM patients and non-rheumatologcial controls
| Myositis (n=65) | Non-rheumatological controls (n=65) | Significance | |
| Osteopenia at LS | 25 (38.5%) | 20 (30.8%) | 0.357 |
| Osteoporosis at LS | 13 (20%) | 6 (9.2%) | 0.082 |
| Osteopenia at NOF | 29(44.6%) | 26 (40%) | 0.542 |
| Osteoporosis at NOF | 12(18.5%) | 6 (9.2%) | 0.119 |
| Osteopenia overall | 29(44.6%) | 28 (43.1%) | 0.860 |
| Osteoporosis overall | 19(29.2%) | 9(13.8%%) | 0.033 |
| Reduced BMD overall | 48 (73.8%) | 37 (56.9%) | 0.043 |
| Occurrence of fragility fracture | None=52 | None=54 | 0.651 |
| Vertebral =5 | Vertebral=4 | ||
| Femoral=1Femoral=1 | Femoral=0 | ||
| Wrist=4 | Wrist=3 | ||
| Other sites=3 | Other sites=3 |
Disclosure of Interests: None declared