fetching data ... 
Background: Juvenile idiopathic arthritis (JIA) may have substantial consequences for quality of life, for instance due to chronic pain, restriction of activities, concern about physical appearance, and treatment protocols that may limit interactions with peers. However, it remains unclear whether children and adolescents with JIA sow a higher incidence of psychiatric disorders compared with the general population.
Objectives: To examine the incidence of psychiatric disorders during childhood in JIA patients in Sweden relative to general population controls.
Methods: We performed a register- and population-based cohort study including new-onset JIA patients aged 0 to 17 years 1 st January 2012 through 31st December 2017. Incident JIA patients were followed-up from the date of their 2 nd JIA diagnosis. At this date, five sex-age-region matched individuals were sampled from the general population. Nine psychiatric disorders were defined with ICD-10 codes and associated drugs (ATC codes): psychotic disorders (ICD-10: F20-29; ATC: N05A), mood and anxiety disorders (F30-F43; N05B, N06A, R06AD01, R06AD02, N03AX16), sleeping disorders (F51; N05C, N03AE01), eating and personality disorders (F50, F60-61, F69), neuropsychiatric disorders (F70-F79, F84, F90; N06BA, C02AC02), substance misuse (F10-F19; N07B), suicide attempts (X60-X84, Y10-34) and death by suicide or substance abuse, and all these combined. The follow-up stopped at date of first outcome, migration, death, 18 th birthday or end of the study period, whichever occurred first. Incidence rates were calculated and compared by Cox regression analyses, adjusted for age, sex, calendar year, patient’s and family’s history of psychiatric disorder, country of birth, parents’ education level, and comorbidities (IBD, obesity and celiac disease). In sensitivity analyses, we (1.) excluded children with a history of a psychiatric diagnosis at start of follow-up, and (2.) defined the psychiatric disorders based on ICD-10 codes only.
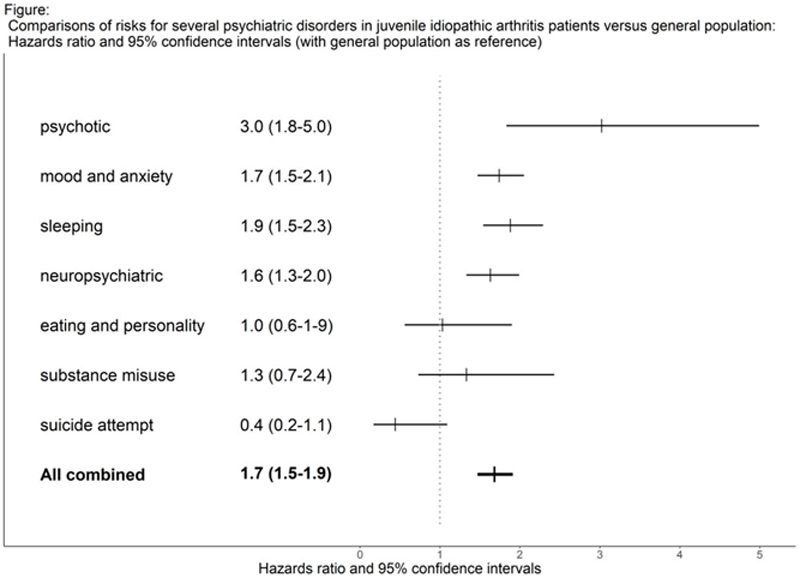
Results: We identified 2224 JIA patients (64% girls, mean age: 9.8 years) and 10,264 matched controls. In the JIA cohort, 309 patients developed a psychiatric disorder (all outcomes combined) during 4998 person-years (pyrs), which corresponded to a crude incidence rate (IR) of 6.2 per 100 pyrs (95% confidence interval (CI): 5.5-6.9). The corresponding crude IR for the general population matched controls was 3.6 (3.4-3.9). Comparing these incidence rates resulted in a sex-age adjusted hazard ratio (HR) of 1.66 (95% CI: 1.46-1.89) and a fully adjusted HR of 1.68 (1.47-1.91). Considering specific outcomes, the IRs per 100 pyrs in the JIA population ranged from 0.1 (suicide attempt) to 3.7 (mood and anxiety disorders) (
Conclusion: The burden of psychiatric illness in individuals with JIA is increased compared to the general population.
Risk of psychiatric disorders in JIA patients and general population controls.
| Disorders | N events JIA | N events controls | IR JIA (95% CI) | IR controls (95% CI) |
| All combined | 309 | 918 | 6.2 (5.5-6.9) | 3.6 (3.4-3.9) |
| Psychotic | 25 | 44 | 0.5 (0.3-0.7) | 0.2 (0.1-0.2) |
| Mood | 194 | 534 | 3.7 (3.2-4.3) | 2.0 (1.9-2.2) |
| Sleeping | 148 | 348 | 2.8 (2.4-3.3) | 1.3 (1.2-1.5) |
| Neuropsychiatric | 126 | 442 | 2.4 (2.0-2.8) | 1.7 (1.5-1.9) |
| Eating | 13 | 55 | 0.2 (0.1-0.4) | 0.2 (0.2-0.3) |
| Substance misuse | 14 | 49 | 0.3 (0.2-0.4) | 0.2 (0.1-0.2) |
| Suicide attempt | 7 | 55 | 0.1 (0.1-0.3) | 0.2 (0.2-0.3) |
IR: crude incidence rate per 100 person-years; CI: confidence interval
1 adjustment: see text.
Disclosure of Interests: Bénédicte Delcoigne: None declared, AnnaCarin Horne Consultant of: SOBI and Novartis, Soley Omarsdottir: None declared, Johan Reutfors: None declared, Johan Askling Consultant of: Abbvie, Astra-Zeneca, BMS, Eli Lilly, MSD, Pfizer, Roche, Samsung Bioepis, Sanofi, and UCB. These entities have entered into agreements with Karolinska Institutet with JA as principal investigator, mainly in the context of safety monitoring of biologics via the ARTIS national safety monitoring system