fetching data ... 
Background: Patients with Rheumatoid arthritis (RA) have an increased risk of infections due to the disease itself, and/or immunosuppressive therapy. The risk of herpes zoster (HZ) including disseminated HZ is also increased (1 )
Objectives: In an unselected series of RA patientswe assess a )prevalence, b )general features and c ) predictive factors of HZ.
Methods: Study of 393 RA patients included in the prospective vaccination program of the Preventive Medicine and Rheumatology department of a University hospital, from October 2011 to October 2016. The minimum follow-up was of 12 months; therefore, it was made until December 2020. HZ vaccination is not included in our vaccination program.
RA was diagnosed according to the ACR/EULAR 2010 criteria. HZ was diagnosed if presented: characteristic skin rash and blisters, paresthesia and local pain, in one (localized) or more dermatomes (generalized).
Information on patients and HZ characteristics was retrieved from the hospital and general physician records.
Results: We studied 393 patients (310 women), mean age 61.5±11.9 years. They were followed-up during a mean period of 82.6±15.2 months(range; 50 months-9 years).
HZ infection was observed in 31 of 393 patients (7.9%) (26 women); mean age 67.5±11.6ys. Prevalence of HZ in this period (122months) was 7.88% with an annual incidence rate of 0.73/100 patients/year. A comparison between patients with and without HZ was performed (
Main features of different groups
| Variables | RA patientsN= 393 | RA with HZN=31 | RA without HZN=362 | PHZ vs noHZ | Variables (continued) | RA patientsN= 393 | RA with HZN=31 | RA without HZN=362 | PHZ vs noHZ |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) (men±SD) | 59.4±12.9 | 64.7±11.8 | 59.1±12.9 | 0.02 | MTX | 365 (92.87) | 29 (93.54) | 336 (92.81) | 0.87 |
| Sex (women)(%) | 309(78.62) | 25 (80.6) | 284 (78.5) | 0.95 | LFN | 127 (32.31) | 12 (38.70) | 115 (31.76) | 0.42 |
| RA Evolution(months) (mean±SD) | 136.9±109.8 | 155.3±117.0 | 135.30±109.2 | 0.33 | SSZ | 94 (23.91) | 7 (22.58) | 87 (24.03) | 0.78 |
| Hypertension, n(%) | 165 (42.0) | 19 (61.3) | 146 (40.3) | 0.04 | Anti-TNFa, n (%) | ||||
| Diabetes Mellitus, n(%) | 55 (14.0) | 7 (22.6) | 48 (13.3) | 0.24 | ADA | 144 (36.6) | 15 (48.4) | 129 (35.6) | 0.22 |
| Dislypidemia, n(%) | 149 (37.9) | 15 (48.4) | 134 (37.0) | 0.29 | ETN | 139(35.4) | 16 (51.6) | 123 (33.9) | 0.05 |
| RAfeatures, n(%) | IFX | 40 (10.1) | 5 (16.1) | 35 (9.7) | 0.25 | ||||
| PositiveRF | 224 (57.0) | 17 (54.8) | 207 (57.2) | 0.95 | GLM | 33 (8.4) | 3 (9.7) | 30 (8.3) | 0.74 |
| PositiveACPA | 207 (52.7) | 13 (41.9) | 194 (53.6) | 0.29 | CZP | 13 (3.3) | 1 (3.2) | 12 (3.3) | 0.97 |
| Erosions | 145 (36.9) | 10 (32.3) | 135 (37.3) | 0.71 | Non anti-TNFa n (%) | ||||
| Subcutaneousnodules | 22 (5.6) | 1 (4.6) | 21 (5.8) | 0.85 | TCZ | 134 (34.1) | 16 (51.6) | 118 (32.6) | 0.05 |
| Pulmonary fibrosis | 20 (5.1) | 3 (9.7) | 17 (4.7) | 0.20 | RTX | 69 (17.5) | 9 (29.0) | 60 (16.7) | 0.13 |
| Associated Sjögren Syndrome | 20 (5.1) | 1 (3.2) | 19 (5.3) | 0.95 | ABA | 55 (13.9) | 6 (19.3) | 49 (13.5) | 0.41 |
| Vasculitis | 23 (5.9) | 2 (6.5) | 21 (5.8) | 0.7 | SARI | 2 (5.1) | 1 (3.2) | 1 (0.3) | 0.03 |
| RATreatment, n (%) | JAK inhibitors n (%) | ||||||||
| Prednisone | 139 (35.4) | 19 (61.3) | 120 (33.1) | 0.04 | BARI | 32 (8.14) | 3 (9.67) | 29 (8.01) | 0.73 |
| Prednisona>5mg/d | 13 (3.30) | 5 (16.1) | 8 (2.20) | 0.001 | TOFA | 17 (4.32) | 3 (9.67) | 14 (3.87) | 0.14 |
| ConventionalDMARDs | UPA | 4 (1.01) | 1 (3.22) | 3 (0.83) | 0.20 | ||||
HZ locations were intercostal (n=6), dorsal (5), abdominal (3), lumbar (3), facial (3), cervical (1), gluteus (1), submmamary fold (1), intermmamary fold (1) and upper extremity (1). Main HZ complications were post-herpetic neuralgia (n=7), visual alteration in facial HZ (n=1) and disseminated HZ(n=1).
HZ treatment was anitiviral agents (n=23) (brivudine=7; acyclovir 6; famciclovir6; valaciclovir4), topic (n=2) and none (n=6).
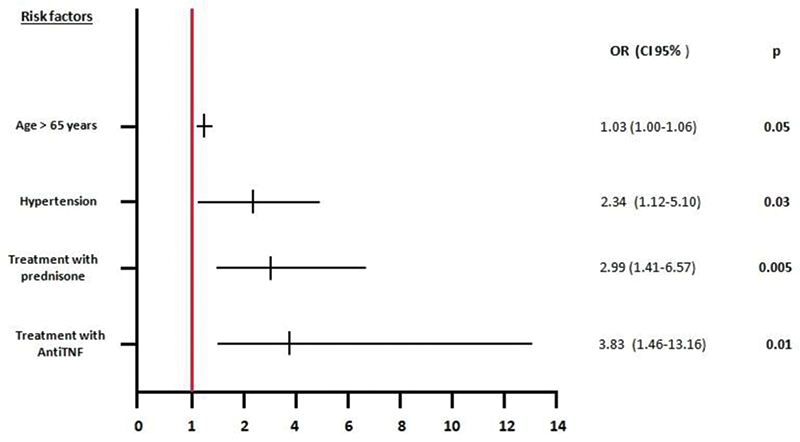
Predictive factors for HZ(
Predictive factors for Herpes zoster
Conclusion: HZ is a relative frequent complication of RA. In our series, although are usually localized, post-herpetic neuralgia is relatively frequent. Probably to include HZ vaccine in our vaccination program of RA may be useful.
REFERENCES:
[1]Robert Harrington et al., J Inflamm Res, 2020 14;13:519-531
Disclosure of Interests: None declared