fetching data ... 
Background: Cogan syndrome (CS) is a rare autoimmune disease, mainly occurring among young people, with an incidence rate of <0.11/100000 (100000). CS is mainly characterized by interstitial keratitis, visual loss associated with cochlear vestibular involvement and Meniere type vertigo. It usually involves all systems of the body, and about 10% to 13% of cases have nervous system involvement. Fewer than 400 cases have been reported worldwide ( 1 ). Glucocorticoid is mainly used in acute attack as the basis of treatment, the effect was not satisfactory( 2 ). Here, we report a case of CS with nerve injury as the main manifestation, which was successfully treated by intrathecal injection of methotrexate combined with dexamethasone.
Objectives: CS often involves multiple systems throughout the body and has a poor clinical prognosis. From a review of our patient’s treatment experience, intrathecal methotrexate combined with dexamethasone may be an effective treatment modality for CNS involvement in patients with refractory recurrent Cogan syndrome.
Methods: The clinical manifestation, laboratory test, treatment, and outcome were described.
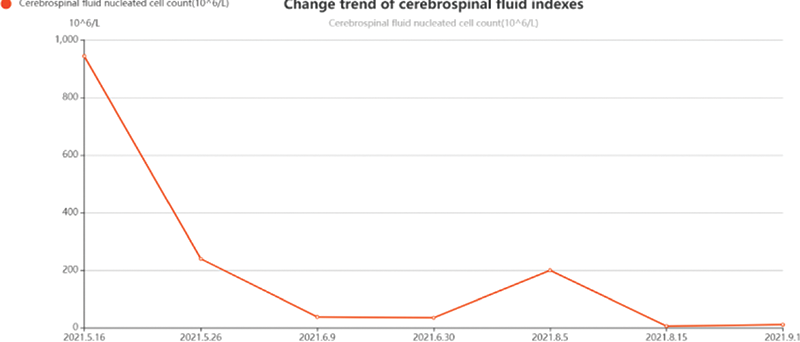
Results: A 31-year-old man presented with recurrent bimanual joint pain for 2 years, after which the patient developed interstitial keratitis, hearing loss and was diagnosed with CS. The patient received treatment with glucocorticoid, cyclophosphamide, methotrexate, tacrolimus, leflunomide, mycophenolate mofetil, hydroxychloroquine, adalimumab. The joint pain was improved, but the headache, dizziness, tinnitus and hearing impairment were significantly aggravated, and syncope occurred. Cerebrospinal fluid examination for lumbar puncture on admission of the patient showed CSF pressure > 185 mmH 2 O, CSF microprotein 1.10 g/l, and CSF nucleated cell count 120x10^6 /L. At the beginning, we successively treated the patient with methylprednisolone (40 mg, QD), gamma globulin (10 g, QD), methotrexate (20 mg, QW) and cyclophosphamide (100 mg, QOD), but the effect was not satisfactory. After excluding infection, we treated this patient with intrathecal methotrexate 10 mg combined with dexamethasone 10 mg, and the patient’s symptoms of dizziness, headache, and tinnitus improved significantly, and his hearing did not decline significantly any more. The patient received a total of seven intrathecal injections (cumulative methotrexate 60 mg + dexamethasone 65 mg) during the subsequent 6 months. His dizziness, headache, tinnitus and other neurological symptoms improved significantly, no further syncope, fever. CSF protein quantification and the number of CSF nucleated cells decreased significantly.
Conclusion: CS patients are often accompanied by multisystem injuries, so it is essential to correctly identify CS and provide appropriate treatment as soon as possible. For patients with neurological involvement who do not respond to treatment with glucocorticoids and immunosuppression, intrathecal methotrexate combined with dexamethasone may be considered as a treatment option for CS in the future.
REFERENCES:
[1]G. M. Espinoza, J. Wheeler, K. K. Temprano, A. P. Keller, Cogan’s Syndrome: Clinical Presentations and Update on Treatment. Curr Allergy Asthma Rep 20 , 46 (2020).
[2]R. Padoan et al. , Cogan’s syndrome: new therapeutic approaches in the biological era. Expert Opin Biol Ther 19 , 781-788 (2019).
Change trend of nucleated cell count in cerebrospinal fluid during treatment
Disclosure of Interests: None declared