fetching data ... 
Background: Patients with chronic inflammatory arthritis (e.g. rheumatoid arthritis; RA) or inflammatory exacerbations of chronic degenerative joint diseases (e.g. osteoarthritis; OA) suffer from recurrent pain, restricted function and reduction of daily activities. The current standard of intraarticular (i.a.) therapy is the injection of steroids, which can increase risk of infection, cartilage degenerations, and other well-known systemic side effects. A novel approach without such complications could be the activation of peripheral opioid receptors, e.g. by i.a. application of small, systemically inactive doses of morphine.
Objectives: The aim of this randomized placebo-and active drug controlled double blind trial was to investigate reduction of pain in chronic knee arthritis patients following i.a. injections of morphine, a standard steroid (triamcinolone), or placebo. The primary hypothesis was that i.a. morphine results in significantly lower pain scores than placebo. The primary outcome parameter was reduction of the Visual Analogue Scale (VAS) pain at day 7.
Methods: Adult patients with chronic knee arthritis because of osteoarthritis (OA) or inflammatory arthritis (IA, rheumatoid arthritis, psoriatic arthritis, spondyloarthritis, oligoarthritis or monarthritis) and a high level of pain (VAS pain ≥ 4 out of 10) at baseline received a single dose of either morphine 3 mg i.a., or triamcinolone 40 mg i.a., or placebo (NaCl 0.9%) i.a., Patients were monitored closely throughout the entire study period with a total of 4 visits over weeks and documented pain in the morning and evening in a patient´s diary. Safety data was collected during the whole study period. P-values were calculated using two-sided T-tests.
Results: 114 patients were screened, 93 were treated and 89 (96%) completed day 7. Of these n= 61 (66%) were diagnosed with OA and n= 32 (34%) with IA 48 (52%) patients were female, mean age was 58.5 (SD 14 years) and mean disease duration 6.7 years (median 2 years, range <1 year – 42 yearss, IQR <1 – 10 years). The mean VAS pain improvement at day 7 for morphine, triamcinolone and placebo was -22.8, -37.7, and -19.8 respectively. The differences were not significant (p=0.69) for placebo vs. morphine, but significant for placebo vs. triamcinolone and for triamcinolone vs. morphine (p=0.013 and p=0.006). Mean improvements of the everyday pain documentation are shown in
Mean VAS pain over one week in patients with chronic knee arthritis treated with morphine, triamcinolone or placebo as a single intraarticular injection.
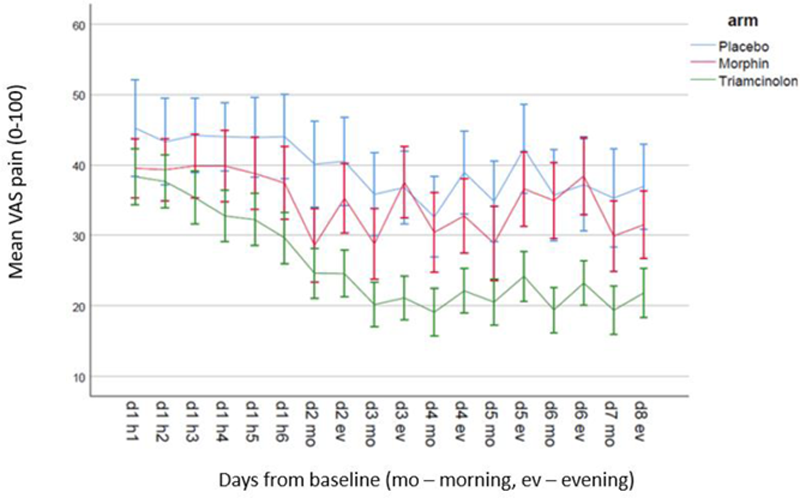
Conclusion: In this randomized, placebo and active controlled double blind trial a single dose of 3 mg i.a. administered morphine did not lead to significant improvements in comparison to placebo and was inferior to triamcinolone at day 7. The same was true during the first 7 days as shown in the pain documentation in patient diaries. These data does not support the use of i.a. morphine for pain reduction in patients with chronic arthritis.
Disclosure of Interests: Hildrun Haibel Speakers bureau: AbbVie, MSD, Janssen, Roche and Pfizer, Consultant of: Roche, Boehringer, Janssen, MSD, Novartis, and Sobi, Grant/research support from: BMBF Neuroimpa 01EC1403F, Joachim Sieper Speakers bureau: Abbvie, Janssen, Lilly, Merck,Novartis, UCB, Consultant of: Abbvie, Lilly, Merck, Novartis, UCB, Denis Poddubnyy Speakers bureau: AbbVie, Bristol Myers Squibb, Eli Lilly, MSD, Novartis, Pfizer, and UCB, Consultant of: AbbVie, Biocad, Eli Lilly, Gilead, GlaxoSmithKline, MSD, Novartis, Pfizer, Samsung Bioepis, and UCB, Grant/research support from: AbbVie, Eli Lilly, MSD, Novartis, and Pfizer, Valeria Rios Rodriguez: None declared, Fabian Proft Speakers bureau: Abbvie, BMS, MSD, Novartis, Pfizer, Roche and UCB, Consultant of: Abbvie, BMS, MSD, Novartis, Pfizer, Roche and UCB, Grant/research support from: Novartis, Judith Rademacher: None declared, Sabrina Igel: None declared, Peter Martus: None declared, Christoph Stein Grant/research support from: BMBF Neuroimpa 01EC1403F.