CELL LINEAGE-SPECIFIC TRANSCRIPT DECONVOLUTION OF SYNOVIAL BIOPSIES FROM THE R4RA TRIAL IDENTIFIES CELL POPULATIONS ASSOCIATED WITH RESPONSE TO RITUXIMAB AND TOCILIZUMAB
F. Rivellese1, C. Cubuk1, A. Surace1, K. Goldmann1, E. Sciacca1, G. Giorli1, A. Nerviani1, L. Fossati-Jimack1, G. Thorborn1, M. Bombardieri1, M. Barnes1, M. Lewis1, C. Pitzalis1, on behalf of R4RA Investigators
1Queen Mary University of London, Centre for Experimental Medicine and Rheumatology, London, United Kingdom
Background: The R4RA trial, the first biopsy-based randomised trial in TNF-i inadequate responder patients with Rheumatoid Arthritis, showed that molecular stratification of RA synovial tissue was associated with clinical response, demonstrating that, in patients with low/absent B-cell lineage signature in synovial-tissue, tocilizumab is superior to rituximab
1
.
Objectives: Here, we aimed to perform cell-transcript deconvolution of pre-and post-treatment synovial biopsies from the R4RA trial.
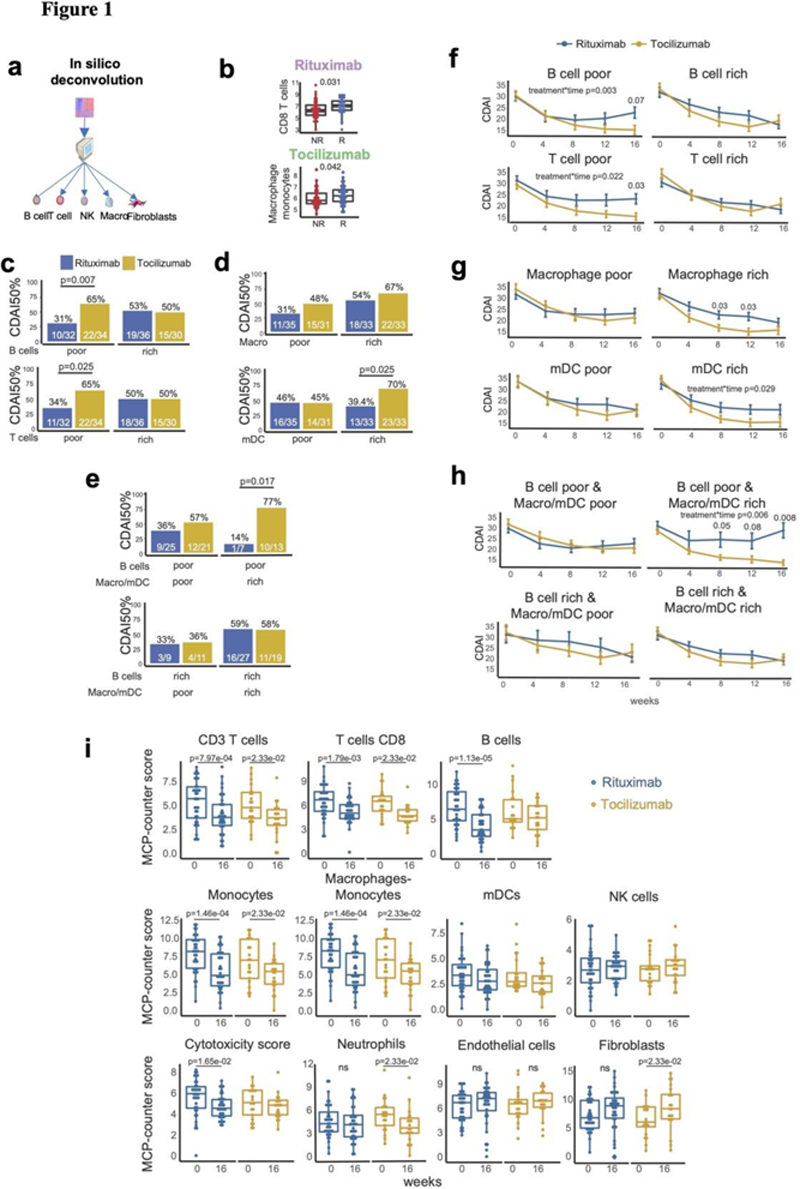
Methods: A total of 164 patients underwent pre-treatment synovial biopsy (US-guided or arthroscopic) prior to randomization 1:1 to rituximab (83) or tocilizumab (81). 65 patients had a repeat biopsy at 16 weeks when clinical response was assessed using Clinical Disease Activity Index (CDAI) 50% improvement. RNA extracted from a minimum of 6 synovial samples/patient underwent RNA-sequencing and the abundance of tissue-infiltrating immune and stromal cell populations was estimated using the Microenvironment Cell Populations-counter (MCP-counter) method (
Figure 1a
).
Results: At baseline, while synovial semiquantitative immunohistochemistry scores did not differ between CDAI50% responders and non-responders, both for rituximab and tocilizumab, MCP-counter analysis showed significantly higher CD8 T-cells in responders to rituximab and higher macrophage-monocytes and myeloid dendritic cells (mDC) in responders to tocilizumab (
Figure 1b
). Moreover, when patients were classified according to MCP-counter scores, B-cell poor patients (MCP-counter B cell score <median value) showed significantly higher response rates to tocilizumab, while no difference was found in B-cell rich patients (
Figure 1c
). In contrast, macrophage and myeloid dendritic cell (mDC) rich individuals showed higher responses to tocilizumab (
Figure 1d
). Combined scores for lymphoid and myeloid cells demonstrated that patients poor in B-cells but rich in macrophages/mDC had a significantly higher response to tocilizumab (77% responders to tocilizumab vs 14% responders to rituximab, p=0.017, OR 16.48, 95%CI 1.29-1000.5) (
Figure 1e
). By analysing disease activity over time from baseline to week 16, we found a statistically significant interaction effect between treatments and time in B-cell poor (p=0.003), T-cell poor (p=0.022), mDC rich (p=0.029) and B-cell poor/Macrophages-mDC rich patients (p=0.006) (
Figure 1f
-g-h). Finally, by applying MCP-counter on matched pre-and post-treatment biopsies, rituximab-treated patients showed a significant reduction of B-cells, T-cells and monocyte/macrophages, while tocilizumab-treated patients showed a significant reduction of monocyte/macrophages, T-cells, but also neutrophils, myeloid dendritic cells and, interestingly, an increase in fibroblast signature (
Figure 1i
).
Conclusion: In silico deconvolution of the synovial tissue identify pre-treatment lymphoid cell lineages associated with response to rituximab and myeloid cells for tocilizumab. The longitudinal analysis of matched pre- and post-treatment synovial biopsies indicated that both medications have an effect on synovial immune cells, but tocilizumab can also affect stromal cells.
REFERENCES:
[1]Humby et al.
Rituximab versus tocilizumab in anti-TNF inadequate responder patients with rheumatoid arthritis (R4RA): 16-week outcomes of a stratified, biopsy-driven, multicentre, open-label, phase 4 randomised controlled trial
Lancet. 2021 Jan 23;397(10271):305-317. doi: 10.1016/S0140-6736(20)32341-2.
Acknowledgements: We would like to thank all patients and the R4RA recruiting centres and principal investigators
http://www.r4ra-nihr.whri.qmul.ac.uk/recruiting_centres.php
We would also like to acknowledge the UK National Institute of Health Research for funding the R4RA trial (grant reference: 11/100/76) and Versus Arthritis for providing infrastructure support through the Experimental Arthritis Treatment Centre (grant number: 20022).
Disclosure of Interests: None declared.
Citation: , volume 81, supplement 1, year 2022, page 56
Session: Rheumatoid arthritis - prognosis and prediction
(Oral Presentations)