fetching data ... 
Background: Intercurrent infections are presumed potential triggers of systemic lupus erythematosus (SLE) disease flares. (1) However, most of the evidence is obtained from a limited number of observational studies, and the results of these studies are conflicting. (2,3)
Objectives: To determine whether intercurrent infections are a risk factor for disease flares in SLE.
Methods: Demographic and clinical characteristics of 203 SLE patients from the Amsterdam SLE cohort were collected at baseline, and at the start of an intercurrent infection that either was or was not followed by a flare within three months. Relevant data regarding infections and flares were collected systematically by chart review. Major and minor infections were defined as, respectively: infections for which hospital admission or intravenous antibiotic therapy was required, and infections (proven or not proven, but highly likely based on clinical symptoms and/or response to therapy) for which hospital admission was not warranted. SLE flares were defined as an increase in disease activity requiring intensification of immunosuppressive therapy. Flares were categorized as major or minor depending on fulfillment of a predefined set of criteria. (4) Incidence rates for infections, flares, and infections followed by a flare within three months were calculated using Poisson regression. Descriptive analyses were performed where appropriate. Proportional hazard models with recurrent events and time-varying covariates were used to estimate the hazard ratio of SLE flares.
Results:
Baseline demographic and clinical characteristics
| Variables | SLE patients (n = 203 ) |
|---|---|
| Sex, Female, n (%) | 184 (91) |
| Age, years (median (IQR)) | 40.0 (32.0 – 47.0) |
| Caucasian ethnicity, n (%) | 137 (68) |
| SLICC/ACR damage index (median (IQR)) | 1 (0 – 2) |
| SELENA-SLEDAI2k (median (IQR)) | 4 (2 – 6) |
| Disease duration, years (median (IQR)) | 6 (1 – 11) |
| History of: | |
| Biopsy proven lupus nephritis, n (%) | 38 (19) |
| Renal insufficiency (eGFR < 45), n (%) | 6 (3) |
| Diabetes mellitus, n (%) | 7 (3) |
| Malignancy, n (%) | 5 (3) |
| Stroke, n (%) | 12 (6) |
| Asplenia, n (%) | 5 (3) |
| Treatment variables: | |
| Glucocorticoids, n (%) | 106 (52) |
| Antimalarials, n (%) | 151 (74) |
| Immunosuppressants, n (%) | 75 (37) |
| NSAIDs, n (%) | 67 (33) |
Estimated cumulative incidence of SLE flares (major and minor) following an intercurrent infection within three months
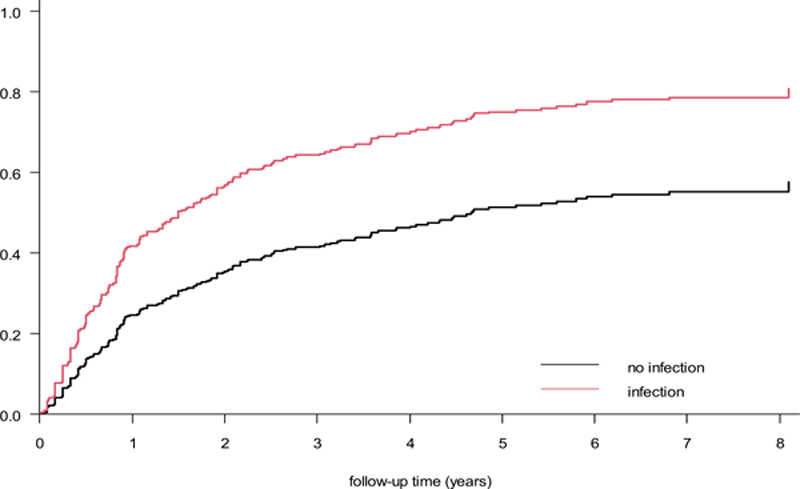
Conclusion: The results of the present study confirm a high frequency of infections in SLE patients and suggest that intercurrent infection is a risk factor for SLE flares. These findings underline the importance of prevention and treatment of infections in SLE patients and create awareness of infections as potential triggers of SLE flares.
REFERENCES:
[1]Fernandez D, et al. Curr. Rheumatol. Rep. 2016;18(3):14.
[2]Bosch X, et al. Lupus. 2006;15(9):584-9.
[3]Tsai PH, et al. Lupus. 2020;29(2):191-8.
[4]Bootsma H, et al. Lancet. 1995;345(8965):1595-9.
Disclosure of Interests: None declared