fetching data ... 
Background: The results from the double-blind BEAT-lupus trial comparing belimumab vs placebo, both after rituximab in systemic lupus erythematosus (SLE) have recently been reported (1). We sought to identify biomarkers of response to belimumab after rituximab to aid a personalised approach to therapy for SLE.
Objectives: To identify biomarkers of clinical response to belimumab after rituximab in the BEAT-lupus trial.
Methods: We constructed a model utilising a range of clinical, routine and exploratory laboratory data, from the BEAT-lupus trial to identify variables at baseline (screening) that could predict a major clinical response (MCR, defined as reduction to BILAG C in all domains, steroid dose of ≤7.5mg/day & SLEDAI≤2, without anti-dsDNA antibody component) at 52 weeks. Relevant serum autoantibodies and cytokines were assayed by ELISA/Simoa, and interferon signatures and BAFF expression measured by RT-PCR. A linear mixed model was applied to longitudinal data collected during the trial stratified by treatment and clinical response. An independent cross-sectional lupus cohort was recruited to validate biomarker association with organ involvement.
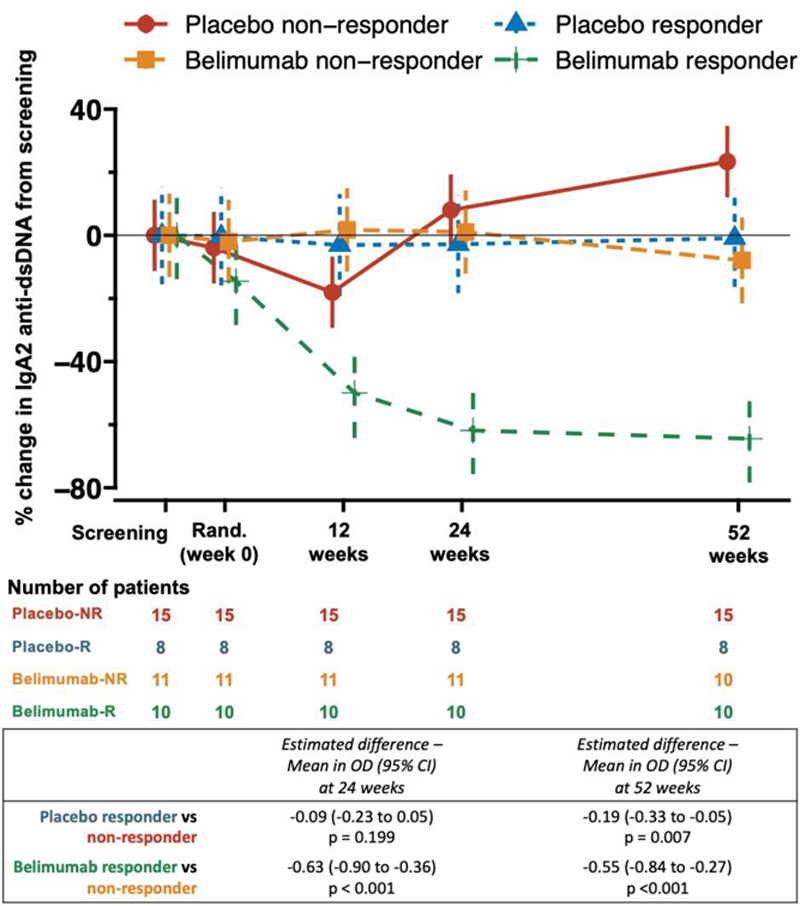
Results: A major clinical response (MCR) was achieved in 48% (10 responders, 11 non-responders) of patients who received belimumab after rituximab compared to 35% (8 responders, 15 non-responders) in the placebo group (i.e. rituximab alone), added to tapered standard of care, at 52 weeks. Baseline serum IgA2 anti-dsDNA antibody levels emerged as the only positive predictor of attaining MCR in belimumab treated patients (AUROC 0.8, 95% confidence interval [CI] 0.7-1.0), but negatively predicted MCR in the placebo arm (AUROC 0.2, CI 0.1-0.4). At baseline, 77% and 85% of patients were positive for serum IgA2 anti-dsDNA antibodies in belimumab and placebo arms respectively, which reduced to 30% at 52 weeks in the belimumab group but remained unchanged with placebo (Fisher exact test, p=0.007). In striking contrast, the percentage of patients who remained IgG anti-dsDNA antibody positive from baseline to 52 weeks were similar between the belimumab and placebo group, despite the serum levels significantly falling in the belimumab group (1). A significant reduction in serum IgA2 anti-dsDNA antibody levels at 24 and 52 weeks from baseline was only observed in belimumab responders (
Percentage change in serum IgA2 anti-dsDNA antibody levels through to 52 weeks stratified by clinical response to belimumab (after rituximab) and placebo (after rituximab) at 52 weeks.
The number of circulating IgA2-secreting (but not total) plasmablasts (p=0.032) and T follicular helper cells (p=0.031) were significantly reduced at 52 weeks in the belimumab treated arm compared to placebo. Elevated serum IgA2 anti-dsDNA antibody levels were also associated with active renal disease irrespective of treatment arm (odds ratio, OR 3.2, CI 1.7-5.8, p<0.001). In contrast, serum IgA1 anti-dsDNA antibody (OR 1.3, CI 1.0-1.7, p=0.042) and interferon-alpha levels (OR 1.4, CI 1.0-2.0, p=0.041), and interferon transcriptional signature (OR 1.1, CI 1.0-1.3, p=0.027) showed a modest association with mucocutaneous disease activity; but did not predict response to B cell targeted therapy. Patients with a high baseline serum IL-6 were less likely to achieve an MCR irrespective of therapy (OR 0.4, CI 0.2-0.9, p=0.033). The associations between serum IgA2 and IgA1 anti-dsDNA antibody levels and active renal and mucocutaneous disease respectively were confirmed in an independent cross-sectional lupus cohort.
Conclusion: IgA2 anti-DNA autoantibodies is a biomarker of response to belimumab after rituximab, and of active renal disease, in systemic lupus erythematosus. Our study reveals distinct molecular networks associated with renal and mucocutaneous involvement, and response to B cell targeted therapies, which could guide precision targeting of current therapies for this heterogenous disease.
REFERENCES:
[1]Shipa M, et al. Annals of Internal Medicine. 2021;174:1647-57.
Acknowledgements: This research was supported by Versus Arthritis (grant number 20873) and the UCLH Biomedical Research Centre (BRC). GSK provided belimumab free of charge, as well as additional funding. GSK had no role in this research and did not have any role during its execution, analyses, interpretation of the data, or decision to submit results. Versus Arthritis and the UCLH BRC reviewed the relevant grant proposals and monitor progress of relevant aspects of the study but did not play any role in the analyses, interpretation of data, or decision to submit results.
Disclosure of Interests: Muhammad Shipa: None declared, Liliana Santos Ribeiro: None declared, Dao Nguyen: None declared, Andrew Embleton-Thirsk: None declared, Mariea Parvaz: None declared, David Isenberg Consultant of: Received consultancy fees from Astra Zeneca, Eli Lilly, Merck Serono, Servier and UCB., Caroline Gordon Speakers bureau: Speakers’ bureau for GSK and UCB, Consultant of: Consultancy work from the Center for Disease Control and Prevention, AbbVie, Amgen, Astra-Zeneca, EMD Serono, MGP, Sanofi and UCB, Grant/research support from: Educational grant from UCB to Sandwell and West Birmingham Hospitals NHS Trust, Michael Ehrenstein Speakers bureau: Speakers’ bureau for GSK, Consultant of: Consultancy work for GSK, Grant/research support from: Part of this research was supported by a grant from GSK to University College London