fetching data ... 
Background: Over the last 20 years aggressive therapy for inflammatory joint diseases (IJD) has become standard of care following the acceptance of Methotrexate as anchor drug and extensive of use biologic therapy since 2003. Immunosuppression increases the risk for common and uncommon infections (1).
Objectives: To compare the temporal rates and associated mortality of hospitalisation with opportunistic infections (OI) (
Methods: All patients hospitalized in Western Australia in the period 1980-2015 with ≥ 2 diagnostic codes for rheumatoid arthritis (RA, n=8490), psoriatic arthritis (PsA, n=601), axial spondylarthritis (AS, n=1419). Overall incidence rates (IR) with microbiologically confirmed OI (Mycobacterial, Fungal and viral infections)(
Diagnostic codes applied to define conditions and opportunistic infections in hospital discharge database.
| ICD9CM | ICD10AM | |
|---|---|---|
| RA | 714.0-714.9 | M05.0-M06.9 |
| AS | 720.0 | M45, M08.10-M08.19 |
| PsA | 696.0 | M07.0-M07.3, L40.5 |
| Tuberculosis | 010.x-018.x | A15–A19 |
| Non-tuberculous mycobacteria | 031.x | A30-A31 |
| Cryptococcosis | 117.5 | B45 |
| Aspergillosis | 117.3 | B44 |
| Histoplasmosis | 115 | B39 |
| All mycosis | 114.0 - 118.9 | B35.0 - B49.9 |
| Pneumocystosis | 136.3 | B59 |
| Cytomegaloviral disease | 078.5 | B25 |
| Influenza | 487.x, 488.x | J09, J10 |
| Herpes zoster | 053.x | B02 |
| Varicella | 052.x | B01 |
Results: The IR for all OI in RA patients (5.19, CI 4.8-5.6) was significantly higher than for PsA (IRR 0.56, CI 0.41-0.76 and AS (IRR 0.64, CI 0.53-0.79) with lower IRR observed especially for tuberculosis and H Zoster in PsA (0,49 and 0,47) and AS patients (0,43 and 0,49). H Zoster, TBC and other mycobacteria were the most frequent cause of OI with cryptococcal and pneumocystis only seen in RA. The IR for TBC decreased over time in RA (R
2
0.51, p=0.08), and AS (R
2
0.47, p=0.09) while the IR for H. zoster decreased in RA only (R
2
0.46, p=0.09) (
Incidence rate per 1000 personyears over time for hospitalisation with opportunistic infections in RA patients.
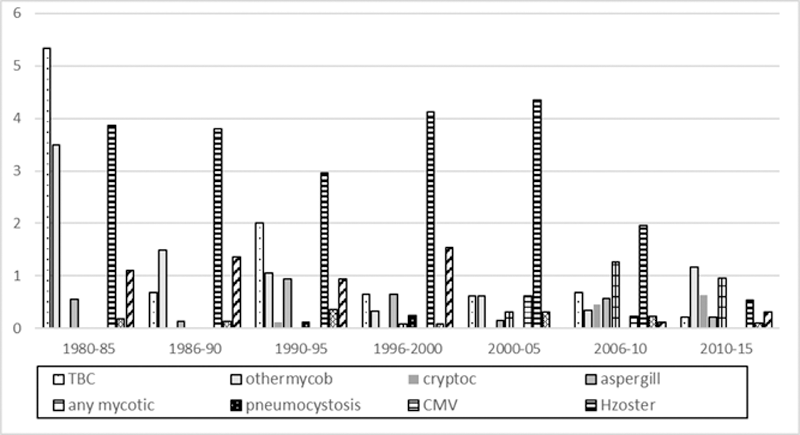
Conclusion: The IR for hospitalization with OI is twice as high for RA patients compared to AS and PsA patients. Admission rates for most OI including have decreased in RA patients over the two decades where more intensive treatment became standard of care. This suggests efficacy of preventative measures. Hospital admission with OI associated with a moderate risk of death, but did not incur a higher risk of death than admission for other medical complications in IJD patients
REFERENCES:
[1]Wang D, Yeo AL, Dendle C, Morton S, Morand E, Leech M. Severe infections remain common in a real-world rheumatoid arthritis cohort: A simple clinical model to predict infection risk. Eur J Rheumatol 2021; 8(3): 133-8.
Acknowledgements: Supported by an unrestricted grant from the Arthritis Foundation of Western Australia.
Disclosure of Interests: None declared