fetching data ... 
Background: Psoriatic arthritis (PsA) is characterized by a range of musculoskeletal and extra-articular disease manifestations. Composite indices are valuable tools to assess the multidimensional nature of PsA. The Psoriatic Arthritis Disease Activity Score (PASDAS) 1 provides robust assessment of both joint and skin domains but is cumbersome to use in clinical practice. The Disease Activity Index for Psoriatic Arthritis (DAPSA) 2 is relatively easy to use but does not assess skin disease.
Objectives: Using pooled data from the phase 3 DISCOVER-1 and DISCOVER-2 studies of guselkumab (GUS) for the treatment of active PsA: 3,4 (1) Describe the rate of achievement of a new composite endpoint combining DAPSA low disease activity (LDA; score ≤14, including remission) and Investigator Global Assessment (IGA) of psoriasis score ≤1 (range=0 [clear] to 4 [severe]); (2) Determine whether earlier (Week [W] 16) DAPSA LDA + IGA ≤1 is predictive of future achievement of minimal disease activity (MDA) or American College of Rheumatology (ACR) 50 response criteria; and (3) Contrast the performance of DAPSA LDA + IGA ≤1 with that of PASDAS LDA (score ≤3.2).
Methods: Patients (pts) with active PsA despite standard therapies (DISCOVER-1: ≥3 swollen + ≥3 tender joints; CRP ≥0.3 mg/dL; ~30% had prior use of up to 2 TNF inhibitors; DISCOVER-2: ≥5 swollen + ≥5 tender joints; CRP ≥0.6 mg/dL; all pts were biologic-naïve) were randomized 1:1:1 to GUS 100 mg at W0, W4, then Q4W or Q8W; or placebo (PBO) with crossover to GUS Q4W at W24. In both studies, efficacy of GUS vs PBO was compared at W24 (primary endpoint). The number (%) of pts with DAPSA LDA + IGA ≤1 was determined at W24 for pts randomized to GUS or PBO. For all GUS-randomized pts, baseline variables associated with DAPSA LDA + IGA ≤1 and PASDAS LDA at W16 and the predictive value of W16 DAPSA LDA + IGA ≤1 or PASDAS LDA for achieving ACR50, MDA, and DAPSA LDA at W52 were assessed using logistic regression models.
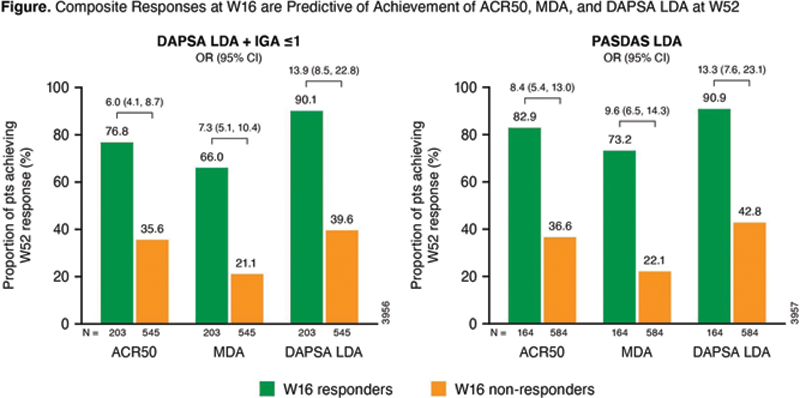
Results: At W24, DAPSA LDA + IGA ≤1 was met by 37% (277/748) of GUS-treated pts vs 13% (48/372) in the PBO group. At W16, 27% (203/748) of GUS-randomized pts had DAPSA LDA + IGA ≤1, and 22% (164/748) had PASDAS LDA. Among the 73% (545/748) of pts who did not have DAPSA LDA + IGA ≤1 at W16, most (77% [418/545]) had IGA ≤1 but not DAPSA LDA; 4% (23/545) had DAPSA LDA but not IGA ≤1, and 19% (104/545) had neither component. Baseline predictors of DAPSA LDA + IGA ≤1 at W16 were male gender, lower dactylitis score, lower Health Assessment Questionnaire-Disability Index (HAQ-DI) score, lower tender joint count (TJC), and higher Psoriasis Area and Severity Index (PASI) score. Baseline predictors of PASDAS LDA at W16 were younger age, lower dactylitis score, lower HAQ-DI score, lower TJC, and higher PASI score. As shown (
Conclusion: DAPSA LDA at W16 predicted future (W52) achievement of the stringent treatment targets of ACR50 and MDA; associations with W52 response were greater when W16 IGA ≤1 was added to DAPSA LDA. DAPSA LDA + IGA ≤1 at W16 as a predictor of W52 ACR50 and MDA response performed similarly to PASDAS LDA. The novel composite of DAPSA LDA + IGA ≤1 may be a reliable predictor of long-term PsA skin and joint response that is more practical to implement than the PASDAS.
REFERENCES:
[1]Helliwell PS et al. Ann Rheum Dis. 2013;72:986-91.
[2]Schoels M et al. Ann Rheum Dis 2010;69:1441-47.
[3]Deodhar A et al. Lancet 2020;395:1115-25.
[4]Mease PJ et al. Lancet 2020;395:1126-36.
Disclosure of Interests: Wolf-Henning Boehncke Speakers bureau: AbbVie, Almirall, Janssen, Leo, Lilly, Novartis, and UCB, Consultant of: AbbVie, Almirall, Janssen, Leo, Lilly, Novartis, and UCB, Alice B Gottlieb Consultant of: AnaptsysBio, Avotres Therapeutics, Beiersdorf, Boehringer Ingelheim, Bristol-Myers Squibb Co., Incyte, GSK, Janssen, LEO Pharma, Eli Lilly, Novartis, Pfizer, Sun Pharmaceutical Industries, Inc., UCB, and Dermavant, Grant/research support from: Boehringer Ingelheim, Incyte, Janssen, Novartis, UCB, Xbiotech, and Sun Pharma, Enrique Soriano Speakers bureau: AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Janssen, Novartis, Pfizer, Roche, and UCB, Consultant of: AbbVie, Janssen, Novartis, and Roche, Grant/research support from: AbbVie, Janssen, Novartis, Pfizer, Roche, and UCB, Alexis Ogdie Consultant of: Abbvie, Amgen, BMS, Celgene, CorEvitas, Gilead, Happify Health, Janssen, Lilly, Novartis, Pfizer, and UCB, Grant/research support from: Abbvie, Pfizer and Novartis and to Forward from Amgen, Olga Ziouzina Consultant of: AbbVie, Amgen, Janssen, Novartis, Eli Lilly, Pfizer, UCB, Celltrion, and Fresenius-Kabi, Emmanouil Rampakakis Consultant of: Janssen, Employee of: JSS Medical Research, Xie L Xu Shareholder of: Johnson & Johnson, Employee of: Janssen Research & Development, LLC, Soumya D Chakravarty Shareholder of: Johnson & Johnson, Employee of: Janssen Scientific Affairs, LLC, May Shawi Shareholder of: Johnson & Johnson, Employee of: Janssen Pharmaceutical Companies of Johnson & Johnson, Marilise Marrache Shareholder of: Johnson & Johnson, Employee of: Janssen Inc, Alexa Kollmeier Shareholder of: Johnson & Johnson, Employee of: Janssen Research & Development, LLC, Atul Deodhar Speakers bureau: AbbVie, Eli Lilly, Janssen, Novartis, Pfizer, and UCB, Consultant of: AbbVie, Amgen, Aurinia, Bristol Myers Squibb, Celgene, Eli Lilly, GlaxoSmithKline, Janssen, MoonLake, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer, and UCB