fetching data ... 
Background: Neuropsychiatric involvement represents one of the most relevant Systemic Lupus Erythematosus (SLE) manifestations and it is characterized by a protean spectrum of clinical disorders. Among them, small fiber neuropathy (SFN) could represent a relevant reason for chronic pain and somatosensorial dysfunctions, even if not included in ACR 1999 nomenclature yet.
Objectives: In the present study we aimed at evaluating the prevalence of SFN among SLE patients with neuropathic pain and identifying significant associations with clinical and laboratory disease features.
Methods: Consecutive SLE patients (according to ACR 1987 criteria), were screened for neuropathic pain through a specific questionnaire (DN4). Subjects were enrolled to the full protocol in the presence of bilateral limb pain and one of the following: hypoesthesia to touch or prick; pain caused or increased by brushing; tingling, numbness and itching; electric shocks, painful cold or burning pain.
We excluded SLE patients with other possible explanation for SFN including diabetes, Sjogren’s syndrome and kidney impairment (eGFR <30 ml/m). For each patient the following data were collected: demographics, medical history, treatments, disease activity (SLEDAI-2K) chronic damage (SLICC damage index ), clinical and laboratory data, including complement level and the main autoantibodies. Each patient enrolled underwent different tools specific for neuropathic pain (such as SFN-SIQ and NPSI), nerve conduction study, quantitative sensory testing (QST) and skin biopsy performed at proximal thigh and distal leg. SFN was diagnosed when intraepidermal nerve fiber density (IENFD) reduction was associated with at least one thermal detection threshold abnormality at QST. A concomitant fibromyalgia (FM) was evaluated by different tools including FIRST, FibroDetect and ACR 2016 criteria.
Results: Among the 114 recruitable subjects, 58 were excluded because of confounding factors and 25 declined the study. Therefore we enrolled 31 patients (M/F 3/28, median age 50.0 years, IQR 21.0; median disease duration 132.0 months, IQR 197.0; median SLEDAI-2k 0, IQR 4 and median SDI 1, IQR 1.2). FM was identified in 81.8% of subjects according to ACR criteria. SFN was diagnosed in 35.5% of patients; among them, in 81.8% a non-length dependent distribution was recognized while in 18.2% a length-dependent pattern and the large fiber dysfunction were found. SFN was associated with anti-Sm (p=0.03), Raynaud’s phenomenon (p<0.01), low complement levels (p=0.04) and SLEDAI-2k≥4 (p=0.04). Neurovegetative symptoms and pain intensity correlated with distal (p<0.001) and slightly with proximal IENFD reduction (p=0.02 and p=0.04). No significant association was found between FM and SFN or IENFD.
Conclusion: The present study suggests that SFN is a common finding in SLE and it should be considered in patient with neuropathic pain, somatosensorial and neurovegetative dysfunctions, especially in subjects with low complement levels, high disease activity and Raynaud’s phenomenon.
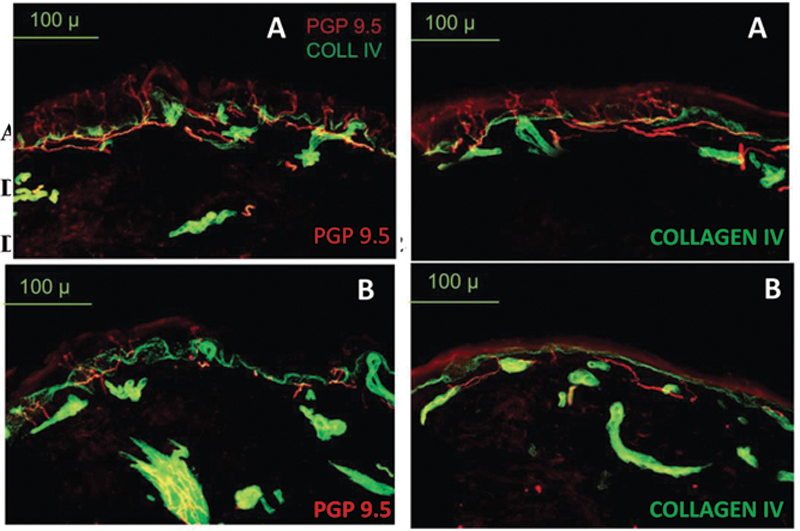
A: SLE patient with normal IENFD. B: SLE patient with low IENFD, consistent with SFN.
Disclosure of Interests: None declared