fetching data ... 
Background: COVID-19 has become a common disease in patients with rheumatic immune-mediated diseases (R-IMID). A risk stratification of the patients at COVID-19 onset is important to predict possible unfavorable results.
Objectives: To identify predictive severity factors in patients with COVID-19 with R-IMID.
Methods: Cross-sectional study in a single University Hospital. We included all consecutive patients with a R-IMID and COVID-19 up to November 6th, 2020. Confirmed infection was defined if the patient had a positive nasopharyngeal swab for SARS-CoV-2.
COVID-19 case severity was divided into mild, moderate, severe and critical according to the United States National Institute of Health (NIH) COVID-19 guidelines (1).
We performed a multivariable analysis and calculated de odds ratio of critical COVID in patients with R-IMID, adjusting by age, sex and comorbidities.
Results: We included 274 patients with R-IMID complicated with COVID-19. At COVID-19 onset, the main comorbidities, analytical values, underlying R-IMID and treatments received are shown in
General features patients with R-IMID and COVID-19
| General features | Overall patients (n=274) | Critical COVID (n=21) | General features (continuation) | Patients (n=274) | Critical COVID (n=21) |
|---|---|---|---|---|---|
| Age, years | 59 ±18 | 76.32 ± 13.4 | Analytical values, mean ± SD | ||
| Female, n (%) | 185 (67) | 11 (52.4) | -CRP (mg/dl) | 4.7 ± 5.25 | 11.7 ± 8.6 |
| CV risk factors, n (% ) | -Creatinine (mg/dl) | 0.91 ± 0.4 | 1.4 ± 0.7 | ||
| -Current smoker | 27 (10) | 2 (9.5) | -Platelets (x103/ul) | 179 ± 78 | 163 ± 72 |
| -Obesity | 49 (18) | 5 (23.8) | -Hemoglobina (g/l) | 13.0 ± 1.8 | 12.5 ± 2.1 |
| -Hypertension | 119 (43) | 18 (85.7) | -Neutrophils (x103/ul) | 4.5 ± 2.5 | 4.9 ± 3.2 |
| -Diabetes Mellitus | 36 (13) | 5 (23.8) | -Lymphocytes (x103/ul) | 1.1 ± 1 | 0.7 ± 0.5 |
| -Dyslipidemia | 119 (43) | 15 (71.4) | -Ferritin (ug/L) | 426 ± 417 | 664 ± 469 |
| Comorbidities, n (% ) | -LDH (U/L) | 257 ± 92 | 314 ± 143 | ||
| -Chronic pulmonary disease | 12 (4.4) | 3 (14.3) | -D-Dimer (ng/ml) | 999±1256 | 1890 ± 1893 |
| -Established cardiovascular disease | 45 (16.4) | 10 (47.6) | Underlying R-IMID, n (% ) | ||
| -Cancer | 21 (8) | 6 (28.6) | -RA | 79 (28.8) | 9 (42.9) |
| -Chronic kidney disease | 27 (10) | 6 (28.6) | -PsA | 55 (20.1) | 3 (14.3) |
| -Chronic liver disease | 11 (4) | 3 (14.3) | -SpA | 34 (12.4) | 0 |
| Treatments received, n (% ) | -PMR | 22 (8) | 6 (28.6) | ||
| -Methotrexate // Hydroxychloroquine | 62 (23) // 50 (18) | 3 (14.3) // 2 (9.5) | -SLE | 22 (8) | 0 |
| -TNFi | 31 (11.3) | 0 | -Vasculitis | 8 (2.9) | 1 (4.8) |
| -Anti-CD20 | 8 (2.9) | 3 (14.3) | -Sjogren’s syndrome | 8 (2.9) | 2 (9.5) |
| -Other biologic DMARDs // JAKINIBs | 16 (5.8) // 6 (2.2) | 1 (4.8) // (4.8) | -Others | 46 (16.8) | 0 |
CRP: C-reactive protein; ILD: Interstitial lung disease; LDH: Lactate dehydrogenase; PMR: Polymyalgia rheumatica¸PsA: Psoriatic arthritis, RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus; SpA: Axial spondyloarthritis
*Adjusted by age, cardiovascular risk factors and comorbidities
According to COVID-19 severity, patients were mild (n=209; 76.3%), moderate (n=35; 12.8%), severe (n=9; 3.3%) and critical (n=21; 7.7%).
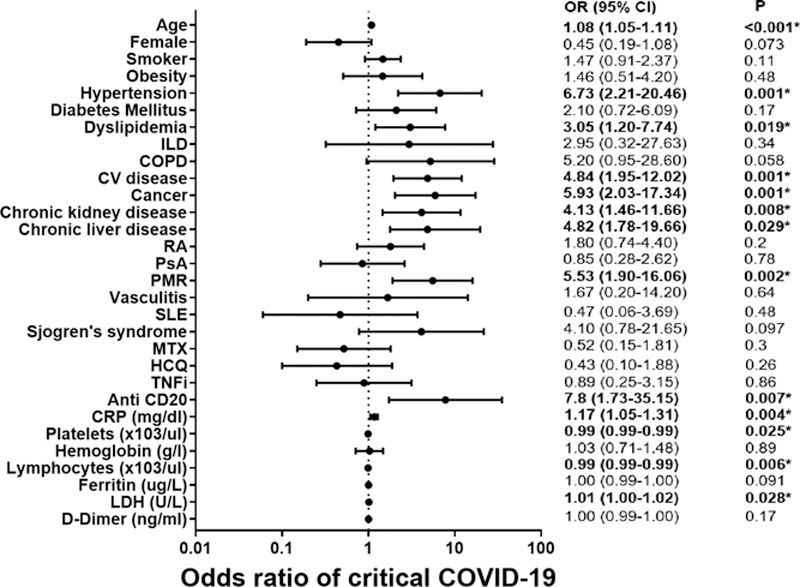
The predictive variables at COVID-19 onset related statistically to critical COVID were older patients, hypertension, dyslipidemia, previous cardiovascular disease, cancer, chronic kidney disease, and chronic liver disease. The only underlying R-IMID and treatment was polymyalgia rheumatica and Rituximab, respectively. Regarding analytical values were higher values of C-reactive protein, LDH, platelets and lymphopenia (
Predictive factors for critical COVID-19 in R-IMID (Multivariable analysis)
COPD: Chronic obstructive pulmonary disease; CRP: C-reactive protein; CV: Cardiovascular; HCQ: Hydroxychloroquine; ILD: Interstitial lung disease; LDH: Lactate dehydrogenase; MTX: Methotrexate; PsA: Psoriatic arthritis; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus; TNFi: TNF inhibitors.
*p< 0.005
Data in graphic are presented in a logarithmic scale.
Conclusion: We identified various factors associated with a worse prognosis of COVID-19 in patients with R-IMID. This can help to identify which patients can present a worse course of the disease at the moment of the diagnosis.
Disclosure of Interests: David Martínez-López: None declared, Iván Ferraz-Amaro: None declared, Diana Prieto-Peña: None declared, Fabricio Benavides-Villanueva: None declared, Cristina Corrales-Selaya: None declared, Lara Sanchez-Bilbao: None declared, Alba Herrero-Morant: None declared, Carmen Álvarez-Reguera: None declared, Martin Trigueros-Vazquez: None declared, Miguel A González-Gay Speakers bureau: Consultation fees/participation in company-sponsored speaker´s bureau from Abbvie, Pfizer, Roche, and MSD, Grant/research support from: Dr. Miguel A. Gonzalez-Gay received grants/research supports from Abbvie, MSD, and Roche, Ricardo Blanco Speakers bureau: Consultation fees/participation in company-sponsored speaker´s bureau from Abbvie, Lilly, Pfizer, Roche, Bristol-Myers, Janssen, and MSD., Grant/research support from: Dr. Ricardo Blanco received grants/research supports from Abbvie, MSD, and Roche