fetching data ... 
Background: Upadacitinib (UPA) was shown to be safe and effective through 2 years in patients (pts) with active ankylosing spondylitis (AS) naïve to biologic disease-modifying antirheumatic drugs (bDMARDs) in the pivotal phase 2/3 SELECT-AXIS 1 trial. 1,2
Objectives: To assess the efficacy and safety of UPA in pts with active AS with an inadequate response (IR) to bDMARDs.
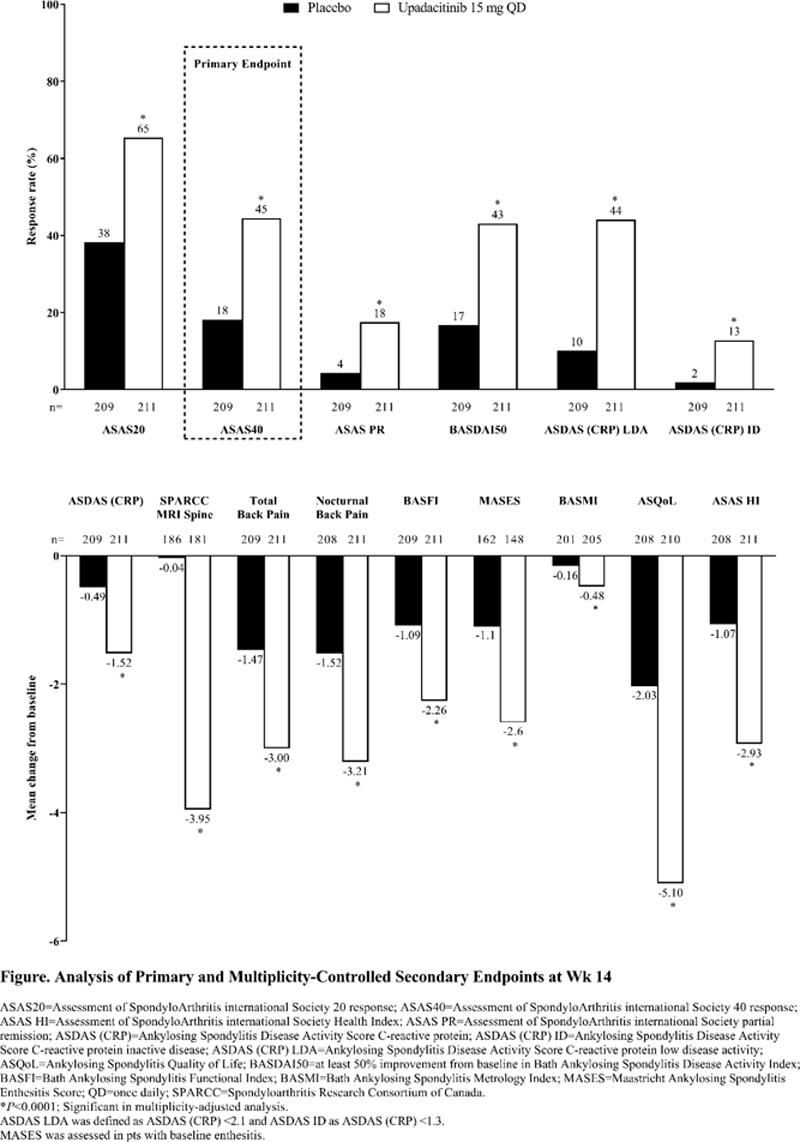
Methods: SELECT-AXIS 2 (NCT04169373) was conducted under a master protocol and includes two separate studies (one for AS bDMARD-IR and one for non-radiographic axial spondyloarthritis [nr-axSpA]). The AS bDMARD-IR study is a randomized, double-blind, placebo (PBO)-controlled, phase 3 trial that enrolled adults ≥18 years with AS who met modified New York criteria, had BASDAI and pt’s assessment of total back pain scores ≥4 (numeric rating scale 0–10) at study entry, and had an IR to one or two bDMARDs (TNF inhibitor or IL-17 inhibitor). Pts were randomized 1:1 to receive oral UPA 15 mg once daily (QD) or PBO during the 14-week (wk) double-blind treatment period. The primary endpoint was ASAS40 response at wk 14. Multiplicity-controlled secondary endpoints evaluated at wk 14 were improvements from baseline in disease activity (ASDAS [CRP], ASDAS ID [<1.3], ASDAS LDA [<2.1], BASDAI50, ASAS20, and ASAS PR), pain (total and nocturnal back pain), function (BASFI), objective measure of inflammation (SPARCC MRI score of the spine), spinal mobility (BASMI), enthesitis (MASES), and quality of life (ASQoL and ASAS HI). Non-responder imputation incorporating multiple imputation (NRI-MI) was used to handle intercurrent events and missing data for binary endpoints. Cochran-Mantel-Haenszel (CMH) test and mixed-effect model for repeated measures (MMRM) were used for analyzing binary and continuous endpoints, respectively. Treatment-emergent adverse events (TEAEs) assessed through wk 14 are reported for pts who had ≥1 dose of study drug.
Results: All 420 randomized pts with active AS received assigned treatment (UPA 15 mg, n=211; PBO, n=209); 409 (97%) received study drug through wk 14. Baseline demographic and disease characteristics were generally similar between treatment groups and reflective of an active AS bDMARD-IR population (74% male; mean age 42.4 years; mean disease duration 7.7 years; 83% HLA-B27 positive; mean BASDAI 6.8). Significantly more pts achieved the primary endpoint of ASAS40 response at wk 14 with UPA vs PBO (45% vs 18%;
P
<0.0001;
Conclusion: UPA 15 mg QD was significantly more effective than PBO over 14 wks of treatment in pts with active AS and IR to bDMARDs. No new safety risks were identified with UPA compared with its known safety profile. 3,4 These findings are consistent with and complementary to those of SELECT-AXIS 1 (bDMARD-naïve AS population), 1,2 and support the use of UPA in pts with active AS, including those who had a previous IR to bDMARD therapy.
REFERENCES:
[1]van der Heijde D, et al. Arthritis Rheumatol . 2021;73(suppl 10).
[2]van der Heijde D, et al. Lancet . 2019;394(10214):2108–2117.
[3]Cohen SB, et al. ARD . 2021;80:304–311.
[4]Burmester G, et al. Rheumatol Ther . 2021;1–19.
Acknowledgements: AbbVie funded this study and participated in the study design, research, analysis, data collection, interpretation of data, review, and approval of the abstract. No honoraria or payments were made for authorship. Medical writing support was provided by Julia Zolotarjova, MSc, MWC, of AbbVie.
Disclosure of Interests: Désirée van der Heijde Consultant of: AbbVie, Bayer, BMS, Cyxone, Eisai, Galapagos, Gilead, GSK, Janssen, Lilly, Novartis, Pfizer, and UCB, Employee of: Director of Imaging Rheumatology BV, Xenofon Baraliakos Speakers bureau: AbbVie, BMS, Celgene, Chugai, Merck, Novartis, Pfizer, and UCB, Consultant of: AbbVie, BMS, Celgene, Chugai, Merck, Novartis, Pfizer, UCB, and Werfen, Grant/research support from: AbbVie, Novartis, Joachim Sieper Speakers bureau: AbbVie, Janssen, Merck, Novartis, Pfizer, Roche, and UCB, Consultant of: AbbVie, Janssen, Lilly, Merck, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Merck, and Pfizer, Atul Deodhar Consultant of: AbbVie, Amgen, Aurinia, BMS, Celgene, GSK, Janssen, Lilly, MoonLake, Novartis, Pfizer, and UCB., Grant/research support from: AbbVie, GSK, Lilly, Novartis, Pfizer, and UCB, Robert Inman Consultant of: AbbVie, Amgen, Janssen, Lilly, Novartis, Pfizer, and Sandoz, Grant/research support from: AbbVie, Amgen, and Janssen, Hideto Kameda Speakers bureau: AbbVie, Asahi-Kasei, BMS, Chugai, Eisai, Janssen, Lilly, Mitsubishi-Tanabe, Novartis, and Pfizer, Consultant of: AbbVie, Janssen, Lilly, Novartis, Sanofi, and UCB, Grant/research support from: AbbVie, Asahi-Kasei, Boehringer Ingelheim, Chugai, Eisai, and Mitsubishi-Tanabe, Xiaofeng Zeng: None declared, Yunxia Sui Shareholder of: May own AbbVie stock or options, Employee of: AbbVie, Xianwei Bu Shareholder of: May own AbbVie stock or options, Employee of: AbbVie, Aileen Pangan Shareholder of: May own AbbVie stock or options, Employee of: AbbVie, Peter Wung Shareholder of: May own AbbVie stock or options, Employee of: AbbVie, In-Ho Song Shareholder of: May own AbbVie stock or options, Employee of: AbbVie