fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a heterogeneous disease which can affect various organs and is characterized by different clinical phenotypes. While the treatment of renal involvement is quite standardized, the therapeutic approach to extra-renal manifestations is subjected to a degree of variability.
Objectives: 1. To describe extra-renal disease flares in terms of clinical phenotype and outcomes in SLE patients 2. To compare data from a real-life setting with a machine learning (ML) approach.
Methods: This study is a retrospective analysis of data from a monocentric cohort of SLE patients who experienced a disease flare between 2015 and 2020. Each flare was followed for one year and was classified according to the organ involvement and categorized according to the BILAG definition of flare. At baseline and at 3,6,12 months the following variables were collected: disease activity (SELENA-SLEDAI score), ongoing therapy and disease state (DORIA definition of remission). Demographic data and previous organ involvement were retrieved from clinical charts. Flares’ features at baseline and during follow up were analyzed in terms of explained variance across the dataset’s Principal Components and clustered with a hierarchical unsupervised learning approach. A ML model based on neural networks was built to early detect flares’ therapeutic difficulty: it was validated after data augmentation to satisfy statistical requirements during the training phase.
Results: 66 extra-renal flares were investigated (
| WHOLE GROUP | MUSKEL | MUCOCUT | CONSTITUTIONAL | CARDIOPULM | HAEMATOL | NEURO | p | |
|---|---|---|---|---|---|---|---|---|
| NUMBER (%) | 66 | 33 (50) | 16 (24.2) | 7 (10.6) | 4 (6.1) | 5 (7.6) | 1 (1.5) | |
| SLEDAI at baseline median (IQR) | 7 (4-29) | 8 (6-10) | 5.5 (4-10) | 5 (4-9) | 9 (4.5-12) | 5 (5-6) | 29 (29-29) | |
| SLEDAI 12 mos median (IQR) | 2 (0-20) | 0.5 (0-4) | 3 (0-4) | 3 (2 – 4) | 0 (0-0) | 2 (0-3) | 14 (14 – 14) | |
| REMISSION 12 mos number (%) | 33 (50) | 21 (63.6) | 5 (31.3) | 4 (57.1) | 2 (40) | 2 (40%) | 1 (100) | 0.217 |
| NON RESPONSE 12 mos number (%) | 17 (25.8) | 8 (25) | 5 (31.3) | 2 (28.6) | 1 (20) | 1 (20%) | 1 (100) | 0.467 |
Flare clusters.
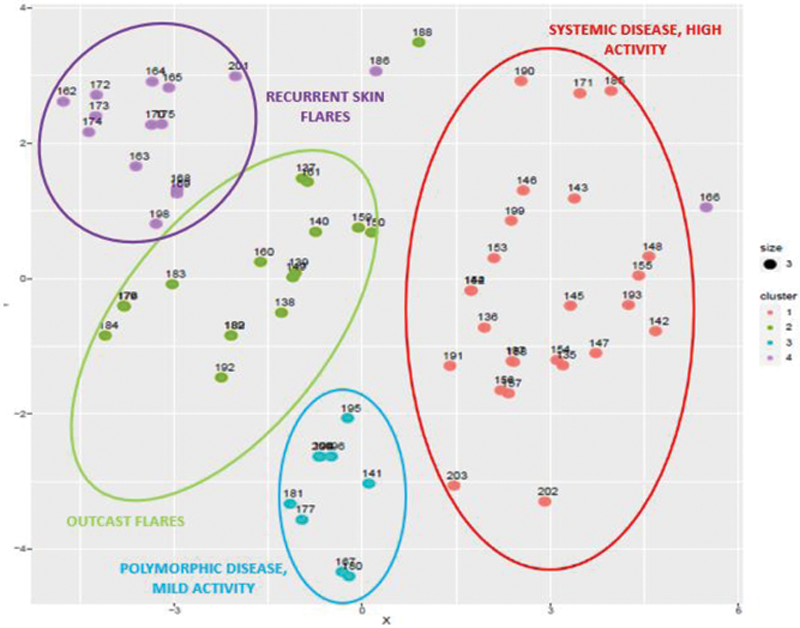
Conclusion: These data suggest that, in a real-life setting, the clinical response rate to therapy of patients with an extra-renal flare is not satisfactory, thus identifying an unmet need in the treatment of SLE and highlighting the absence of a standard treatment. Both the real-life data and the machine learning approach identify flares with MC manifestations as the most difficult to treat with the lower rate of remission after one year. Further prospective studies are necessary to improve the neural network model; ML techniques could help in the early identification of difficult to treat flares to be candidates for new and more aggressive therapeutic strategies for extra-renal manifestations.
Disclosure of Interests: None declared