fetching data ... 
Background: Adult-onset Still’s disease (AOSD) is an autoinflammatory disease characterized by recurrent high fever, rash, joint involvement and hyperinflammation. Although the pathogenesis of the disease is not fully elucidated, some clinical studies have shown that it has a monophasic, polyphasic or chronic persistent course.
Objectives: Seasonal variations in inflammatory rheumatic diseases have been investigated and well-described for many autoimmune diseases, however there is no data regarding AOSD in the literature. Our aim with this study is to evaluate whether there is a seasonal distribution of AOSD and possibly investigate any relationship between this distribution and the course of the disease.
Methods: A total of 62 patients diagnosed with AOSD, according to the Yamaguchi criteria, who were initially diagnosed and followed up in our clinic, were included in this study. The symptoms of the patients until the first diagnosis at our clinic, the season and month in which the symptoms began, demographic data, laboratory findings at diagnosis, and clinical course at follow-up visits were recorded. The relationship between the months that the patients’ symptoms started, and the clinical course was analysed.
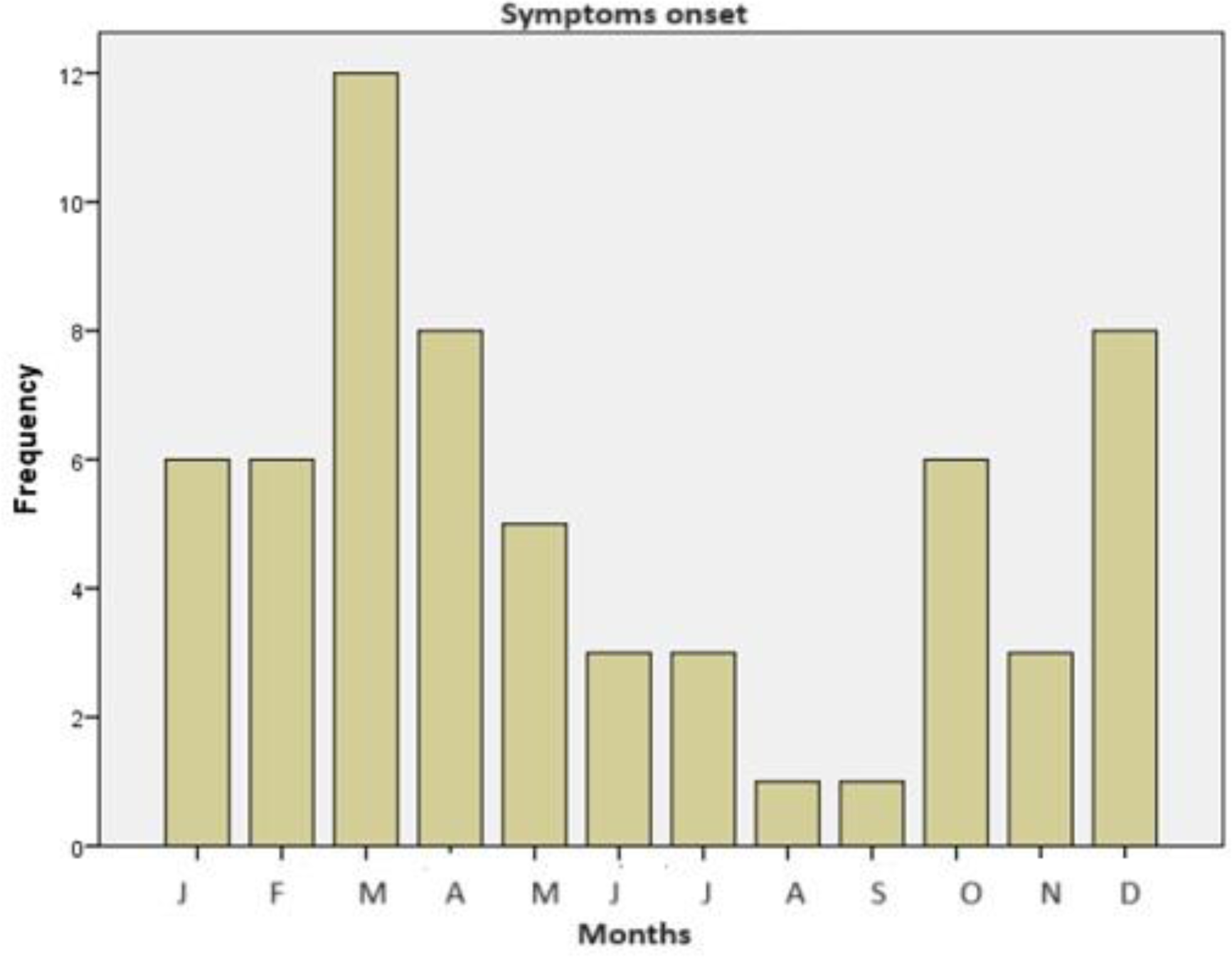
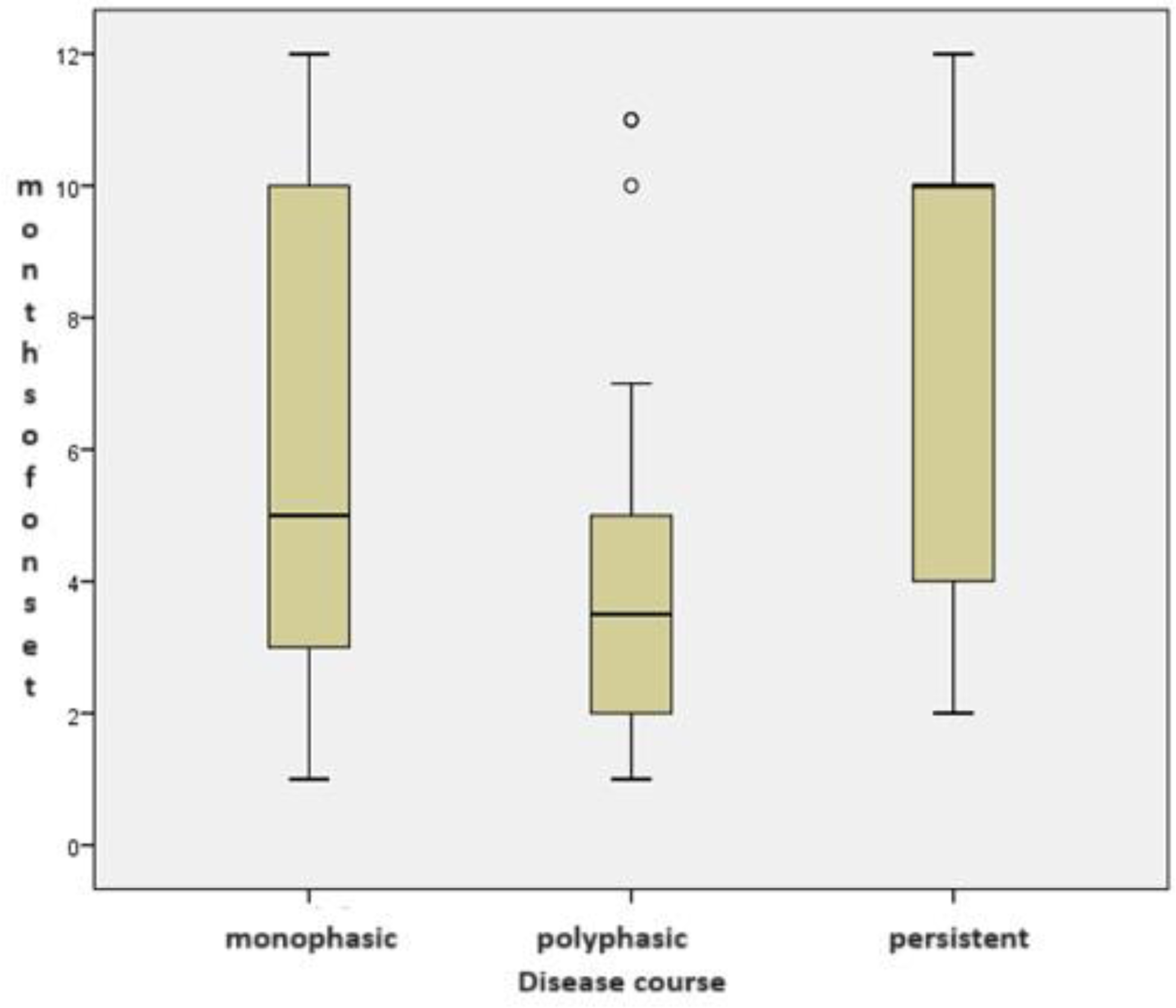
Results: 80.6% of the patients were female and the mean age at diagnosis was calculated to be 40.32 ± 14.88 years. Fever (98.4%), rash (77.4%), arthritis (67.7%) and sore throat (54.4%) were the most common reported clinical findings at diagnosis. Lymphadenopathy (24.2%), splenomegaly (14.5%), hepatomegaly (10%) and serositis (6.5%) were other organ involved. Disease courses were monophasic in 35, polyphasic in 18, and chronic persistent in 5. The total follow-up period was 53.5 ± 57.15 months for the entire cohort. Macrophage activation syndrome (MAS) developed in 6 patients and 2 of these patients died due to multiorgan failure. AOSD onset was most commonly seen in March (19.4%), April (12.9%) and December (12.9%), while Still’s onset was found to be rare in August and September, with 1.6% for each (Figure 1). Among all admissions, AOSD seems to occur most frequently in spring (40.3%) and least frequently in summer (11%). No significant relationship was found between the seasonal distribution of the disease and its clinical course (Figure 2) (p:0.635). It was also found that MAS cases developed in March (2), May (2) and December (2).
Conclusion: Based on some observational studies, infections, drugs, and other environmental factors might induce the disease, having role in the first hit. Seasonal changes along with other reasons, can be a triggering factor. Our study is the first that demonstrates the seasonal distribution in AOSD and investigates any relationship with disease courses. Further studies designed to explore a multifactorial effect are needed in this area.
REFERENCES: [1] Efthimiou P, Kontzias A, Hur P, Rodha K, Ramakrishna GS, Nakasato P. Adult-onset Still’s disease in focus: Clinical manifestations, diagnosis, treatment, and unmet needs in the era of targeted therapies. Semin Arthritis Rheum. 2021 Aug;51(4):858-874. doi: 10.1016/j.semarthrit.2021.06.004. Epub 2021 Jun 13. PMID: 34175791.
[2] Bagnari V, Colina M, Ciancio G, Govoni M, Trotta F. Adult-onset Still’s disease. Rheumatol Int. 2010 May;30(7):855-62. doi: 10.1007/s00296-009-1291-y. Epub 2009 Dec 18. PMID: 20020138.
[3] Ruscitti P, Giacomelli R. Pathogenesis of adult onset still’s disease: current understanding and new insights. Expert Rev Clin Immunol. 2018 Nov;14(11):965-976. doi: 10.1080/1744666X.2018.1533403. Epub 2018 Oct 12. PMID: 30295095.
Acknowledgements: NIL.
Disclosure of Interests: None declared.