fetching data ... 
Background: Rheumatoid Arthritis (RA), the prototype of chronic systemic inflammatory diseases, has a
mortality of 1.3 to 3 times higher than the general population, where cardiovascular
mortality is 40-50%. Now, we know there are increased risk of heart attack (RR: 2.0 - 2.13)
and cerebrovascular stroke (RR: 1.48 - 1.94), considering cardiovascular disease as an extra-
articular manifestation of RA, being independent risk factor of the traditional, with a high
risk of cardiovascular disease (OR: 1.5 – 4.0). This led to the search for additional tools that
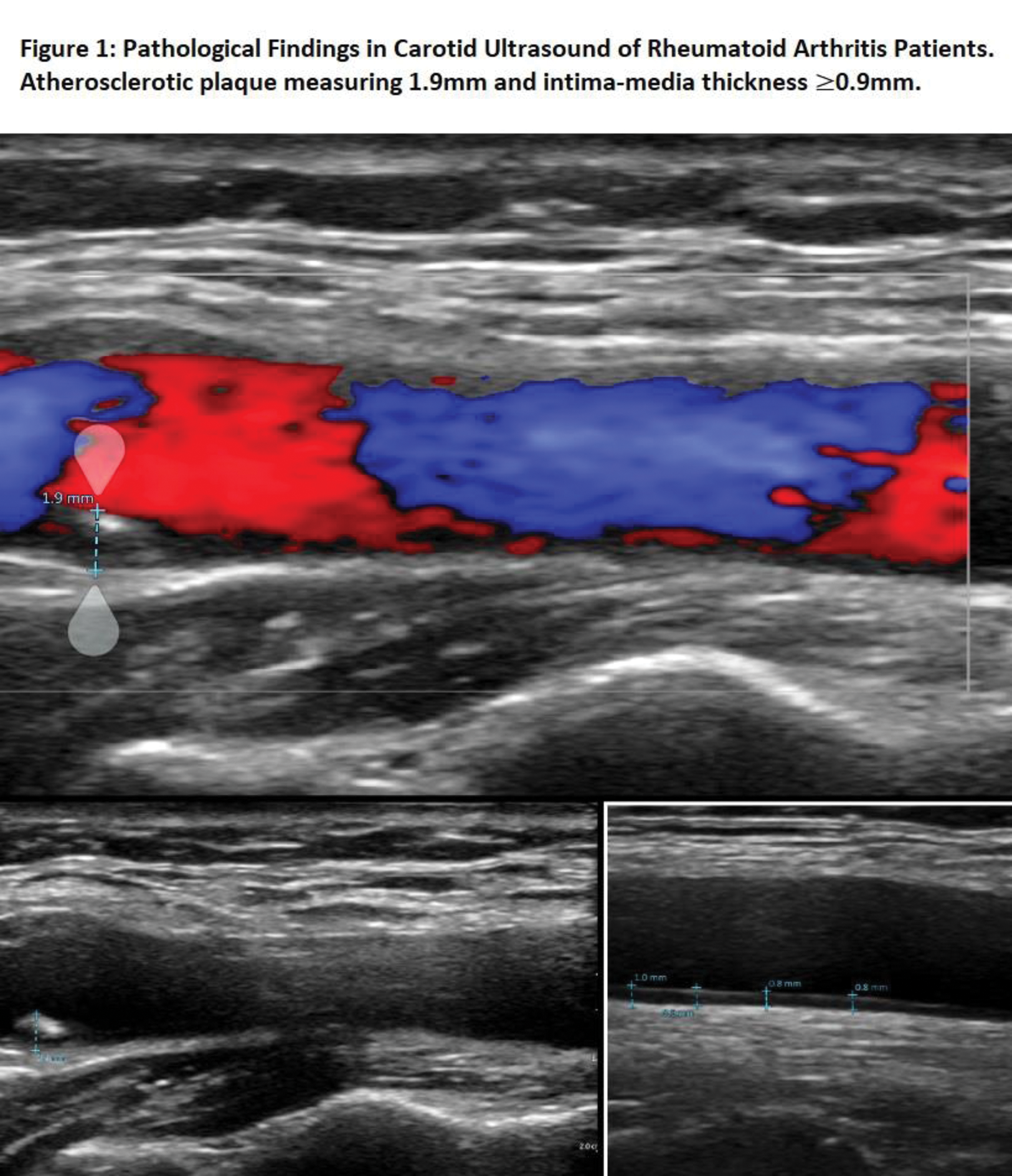
help to identify the cardiovascular risk more accurately. Currently, the use of carotid
ultrasound has been the best option, considering that the measurement of the carotid
intima-media thickness and the presence of atheromatous plaques (AP) a non-invasive
method and surrogate marker of subclinical arteriosclerosis.
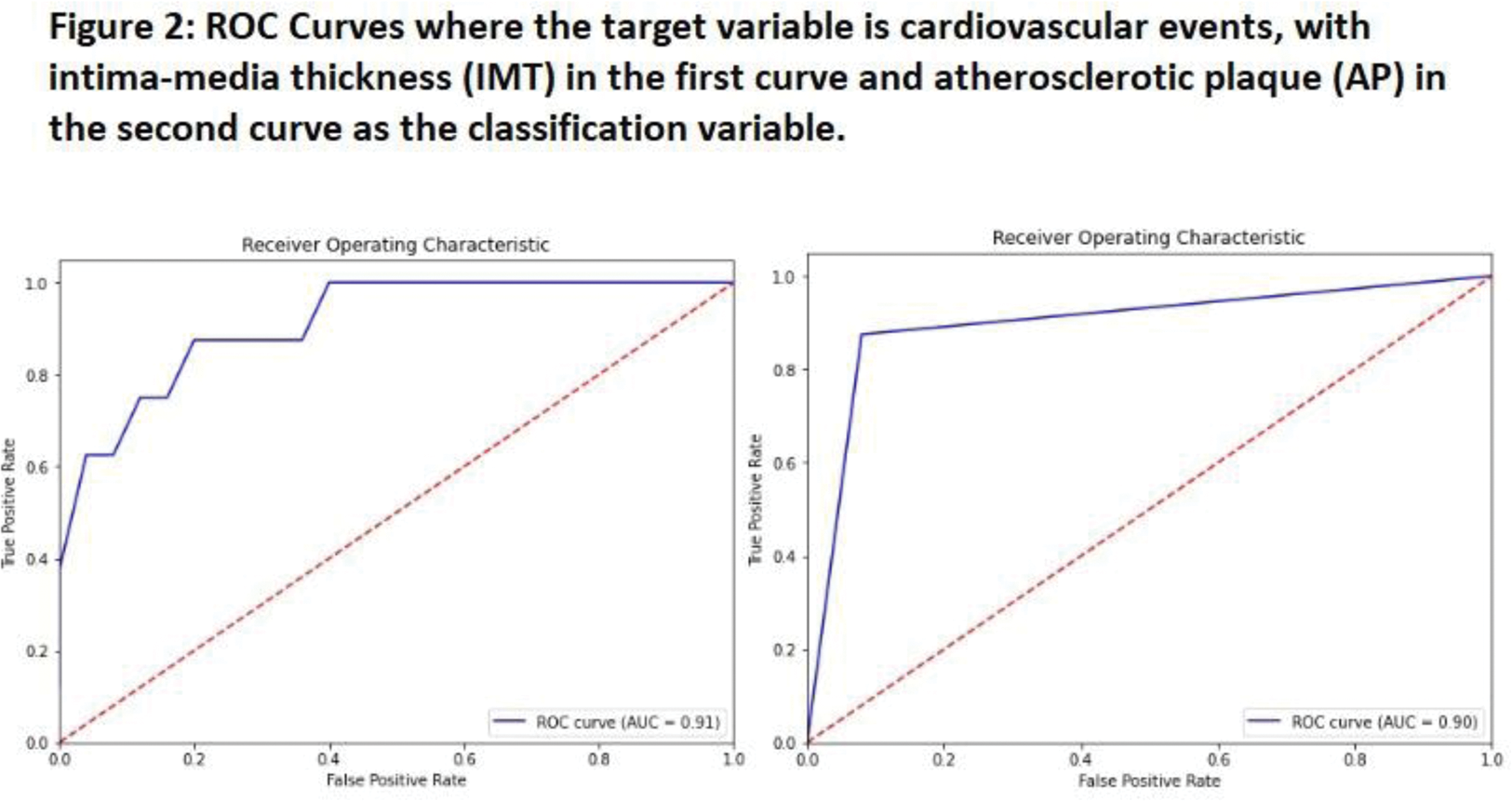
Objectives: Establish if the findings of subclinical arteriosclerosis by carotid ultrasound can be a good predictor of the development of cardiovascular events in a cohort of patients with RA at 10 years.
Methods: A cohort of patients with RA treated in the rheumatology outpatient of a hospital in Castilla La Mancha (Ciudad Real) was evaluated during the year 2013. A prospective evaluation was carried out for the development of CV events over the 10 years and their correlation with the previous ultrasound findings of IMT and PA.
Results: 8 (24%) patients presented a cardiovascular event. 3 (9%) heart failure, 3 (9%) cerebrovascular stroke, and 2 (6%) ischemic heart disease. RA patients who developed CVD had a higher IMT (0.97±0.08) compared to the rest of RA patients who did not have CV complications (0.74±0.15). (p=0.003). The presence of an IMT > or= 0.9mm and atheromatous plaque presented a relative risk of 12.25 (p 0.012) and 18.66 (p 0.003), respectively, for the development of a cardiovascular event.
Conclusion: Carotid ultrasound in patients with RA could allow early detection of subclinical atherosclerosis before the development of CVD, with IMT > or = 0.9mm being the finding most associated with CVD and not influenced by age.
REFERENCES: [1] Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002;
105:1135-43.
[2] Toledano E, Candelas G, Rosales Z, Martínez-Prada C, León L et al. A meta-analysis of
mortality in rheumatic diseases. Reumatol Clin. 2012;8:334–41.
[3] Maradit-Kremers H, Crowson CS, Nicola PJ, Ballman KV, Roger VL, Jacobsen SJ et al.
Incresed unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: a
population based cohort study. Arthritis Rheum. 2005; 52: 402 – 11.
[4] Pieringer H, Pchiler M. Cardiovascular morbidity and mortality in patients with
rheumatoid arthritis:vascular alterations and possible clinical implications. Q J Med. 2011;
104: 13-26.
[5] Micha R, Imamura F, Wyler von Ballmoos M, Solomon DH, Hernán MA, Ridker PM et
al. Systematic review and meta-analysis of methotrexate use and risk of cardiovascular
disease. Am J Cardiol. 2011; 108: 1362-70.
[6] Provan SA, Semb AG, Hisdal J, Stranden E, Agewall S, Dagfinrud H,et al. Remission is
the goal for cardiovascular risk managment in the patients with rheumatoid arthritis: a cross-
sectional comparative study. Ann Rheum Dis. 2011; 70: 812-7.
[7] Gkaliagkousi E, Gavriilaki E, Dounmas M, Petidis K, Aslanidis S, Stella D.
Cardiovascular risk in rheumatoid arthritis: pathogenesis, diagnosis and management.
Journal of Clinical Rheumatology. 2012; 18: 422-30.
[8] Ráček V, Němec P. Rheumatoid arthritis - an independent risk factor for
cardiovascular disease. Vnitr Lek. 2012;58:834-8.
[9] Peters MJ, Symmons DP, McCarey D, Dijkmans BA, Nicola P, Kvien TK, et al. EULAR
evidence-based recommendations for cardiovascular risk managment in patiens with
rheumatoid arthritis and other forms of inflamatory arthritis. Ann Rheum Dis. 2010; 69: 325-
31.
Acknowledgements: NIL.
Disclosure of Interests: None declared.