fetching data ... 
Background: Osteoarthritis (OA) is highly heterogeneous disease and a personalized therapeutic approach is needed to each specific subgroups of patients. When conservative measures fail, surgical intervention, mainly total knee replacement (TKR), is the ultimate recourse. However, a lack of consensus exists over the knee OA (KOA) functional state or burden of the diseases that indicates a TKR surgery. Accordingly, TKR is one of the medical practices with the largest variation among geographical regions [1] .
Objectives: To evaluate the variables influencing TKR decision, recognizing the intricate interplay of factors in the context of KOA.
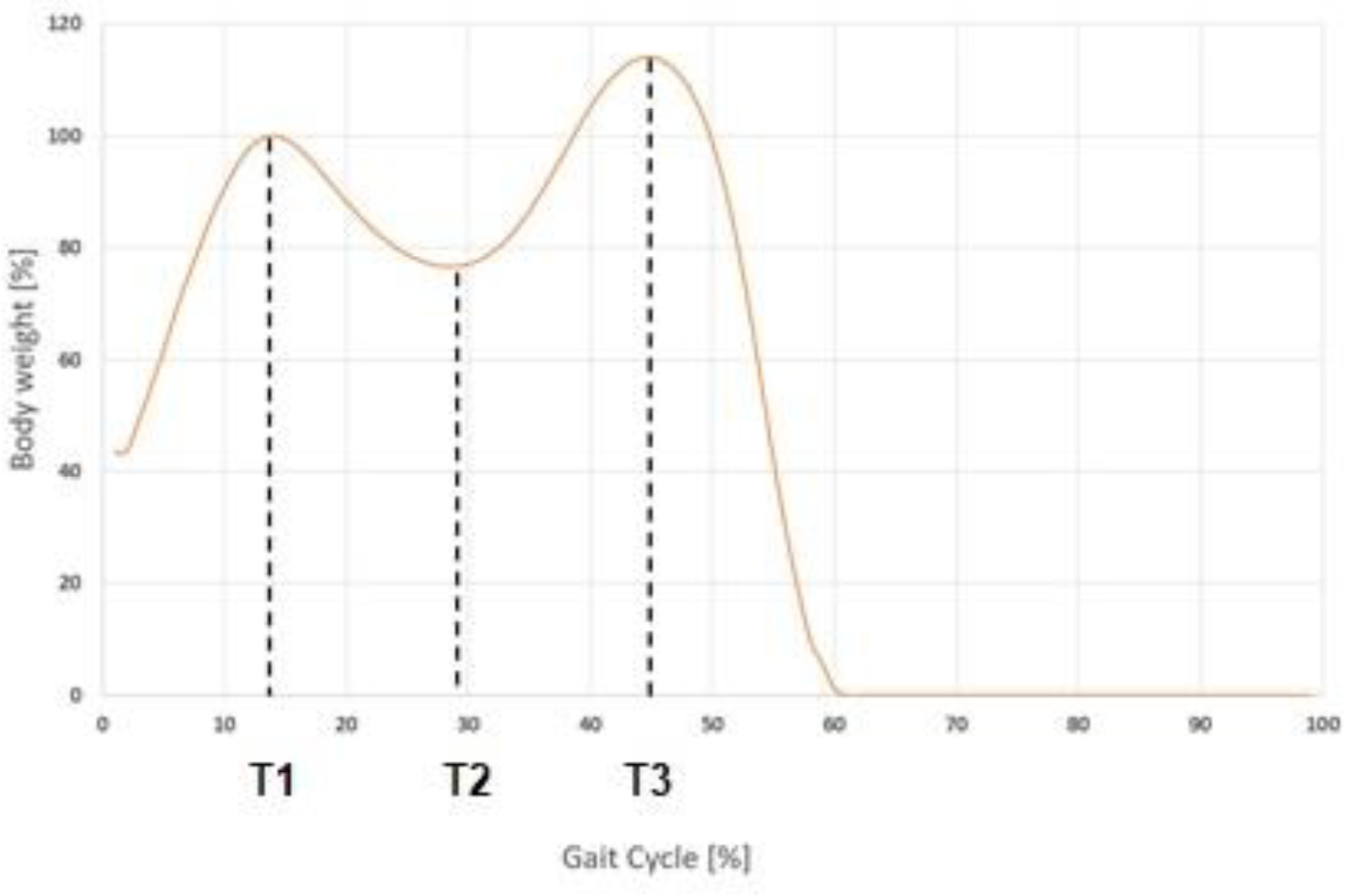
Methods: Primary KOA patients, graded as 2-3 by KL scale, were recruited, stratified based on three key KOA risk factors—gender, age, and BMI—alongside the pivotal decision regarding TKR. However, data regarding different spheres described to play a role in OA aetiology were recorded: 1) Pain (by several questionnaires including WOMAC, Hospital Anxiety and Depression Scale (HAD), Pain Catastrophizing Scale (PCS), central sensitization), 2) Function (daily physical activity (Household and Hobbies & sport), modified-Baecke questionnaire in elderly subjects; 3) joint alignment (knee angles at 3 points of a gait (Figure 1), maximum and minimum, performed using 8 cameras BTS Smart-DX 700, and following Helen Hayes marker protocol); 4) Inflammation (synovial hypertrophy and synovial effusion (SE), measured by ultrasonography). The inherent heterogeneity of the patient population hindered the attainment of complete strata. so, generalized linear mixed-effects models were performed, as it allows to control the bias caused by the uncompleted groups, and strata have been used as random effects, to control the type I error and have an adequate power [2] . First step consisted in selecting the univariate models that presented a significant explanatory variable (p-value<0.05) in order to include them in the multivariate model. Secondly, model refinement involving stepwise elimination of non-significant variables (one at a time), ensuring a reduced AIC compared to the preceding model. Calculations were performed with R version 2023.03.0. The glmer function from the lme4 library was used to perform mixed effect regression analyses [3] .
Results: The final study cohort consisted of 87 patients, 51 women (25 in the CNV group and 26 in the TKR group) and 37 men (23 in the CNV group and 13 in the TKR group). For patients presenting OA in both knees only one of them was assessed, selected randomly.
From the initial 21 variables, only 9 were associated with the treatment decision: angles in the flexion- extension (FE) (T1, and max), adduction-abduction (AA) (T1, T2, T3 and min), WOMAC, PCS, and SE. However, after studying the correlation and the multicollinearity of this variables, only WOMAC, SE and AAT2 angle were included in the model. Therefore, the final model for classifying TKR decision was:
Group i =4.518-0.060(WOMAC i )-0.035(SE i )+0.122(AAT2 i ) +U i +V i +W i +ε i
where Group is the decision to undergo TKR; U, V and W are the random effects for the stratification factors (gender, age and BMI) that follow a normal distribution centred at 0 and with standard deviation X, Y, and Z, respectively; and ε are the residuals. The standard errors of the model coefficients are 1.089, 0.016, 0.020 and 0.054, respectively.
Conclusion: This study provides valuable insights into the clinical determinants influencing the decision for TKR in KOA. The refined predictive model, incorporates variables related to different OA phenotypes previously described 4 : pain (WOMAC), inflammation (SE) and joint alignment (knee angle), offering a nuanced understanding of the decision-making process. This should help collaborative decision-making approach, optimizing patient outcomes and satisfaction.
REFERENCES: [1] Ward MM, et al. JAMA Netw Open. 2020;3(4):e203717.
[2] Kahan, B. C., et al. BMC Medical Research Methodology . 2013, 13(1).
[3] Bates D, et al. Accessible via
[4] Deveza LA, et al. Clin Exp Rheumatol. 2019 Sep-Oct.
Vertical ground reaction force during a gait cycle. The three dashed lines identify the three points of analysis.
Acknowledgements: Project “ PID2021-126469OB-C22”, funded by MCIN/AEI/10.13039/501100011033/ and co-funded by European Union (ERDF, “A way to make Europe”).
Disclosure of Interests: None declared.