fetching data ... 
Background: Rheumatoid arthritis (RA) is a chronic autoimmune disease caused by genetic and environmental factors characterized by joint inflammation. The JAK-STAT inhibitors (jakinibs) are among the therapeutic options together with conventional and biological Disease Modifying Antirheumatic Drugs (DMARDs) [1] .
Objectives: To determine the impact of jakinibs in monocyte and Natural Killer cells (NK) subsets in RA patients by flow cytometry.
Methods: A total of 51 patients treated with jakinibs were recruited, 20 healthy donors and 20 RA patients treated with biological DMARDs, both paired by sex and age with the jakinibs group, were enrolled as controls. Peripheral blood mononuclear cells (PBMCs) were isolated by density gradient using Ficoll. Multiparametric flow cytometry was performed for immunophenotype characterization of different subsets of NK cells acquired in DX Flex cytometer (Beckman Coulter).
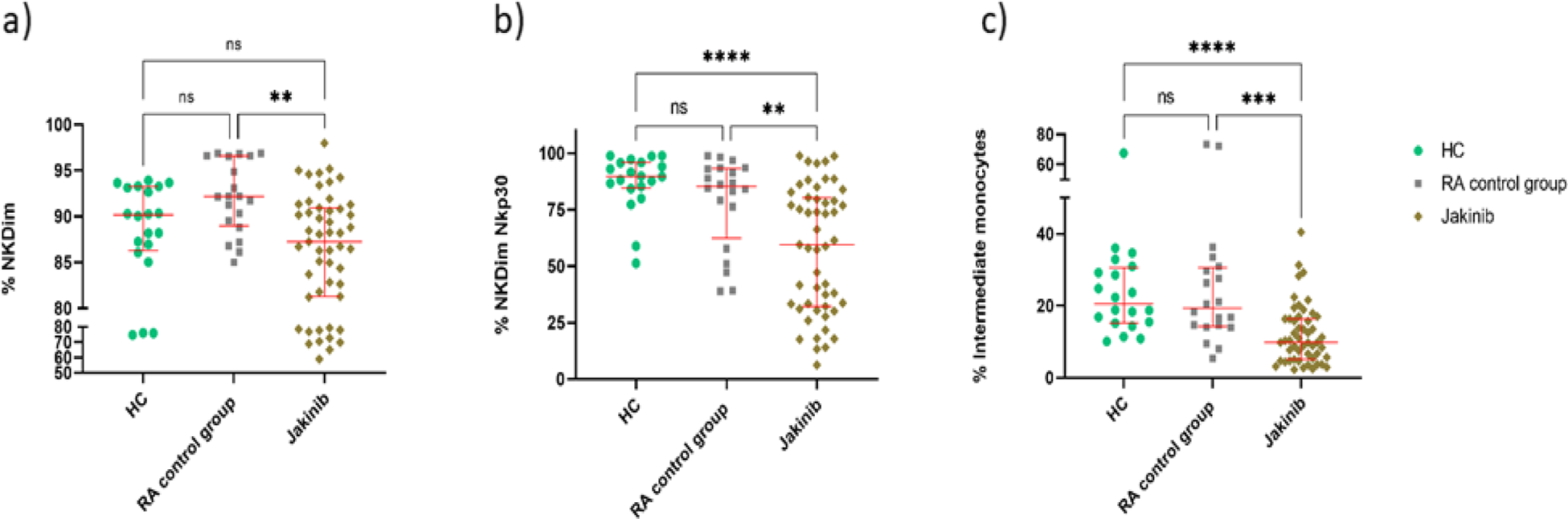
Results: Within the jakinib group, 22 (43.14%) patients were treated with baricitinib (Bari), (27.45%) 14 with tofacitinib (Tofa), 11 (21.57%) with filgotinib (Filgo) and 4 (7.84%) with upadacitinib (Upa); whereas in the RA control group: 11 patients were treated with tocilizumab and 9 treated with abatacept. A significant decrease in the percentage of cytotoxic NK Dim (CD56+CD16+) subset was observed in the jakinib group in comparison to the RA control group (92.18 (89.18-96.59) vs 87.28 (81.29-90.93) p=0.001). There were significant differences between jakinib group and both healthy and RA control groups in the percentage of activated NK Dim expressing Nkp30 (59.51 (32.19-80.34), 89.74 (84.81-95.81) and 85.28 (67.08-93.16), respectively; p values: <0.0001 and 0.007). In addition, the percentage of intermediate monocytes (CD14+, CD16+) was decreased in jakinib group in comparison with RA and healthy controls (9.84 (5.12-16.36), 19.41 (14.39-30.30) and 20.55 (15.34-30.09), respectively; p values: 0.001 and <0.0001).
Conclusion: The JAK-STAT inhibition by jakinibs affects innate cells in a different way than biological DMARDs do. The decrease in both the cytotoxic activated NK subset and intermediate monocytes could explain some of the side effects caused by these drugs related to intracellular threats such as viral infections or possible neoplasia appearances. Further functional studies should be addressed to better understand the impact of jakinibs in innate cell subsets and their relationship with adverse effects in RA patients.
REFERENCES: [1] Meudec L, Richebé P, Pascaud J, Mariette X, Nocturne G. Janus kinase inhibitors alter NK cell phenotypes and inhibit their antitumour capacity. Rheumatology (Oxford). 2023 Aug 1;62(8):2855-2863. DOI: 10.1093/rheumatology/keac710. PMID: 36583542.
Dotplots depicting the percentage of NK Dim cells (a), NK Dim Nkp30 cells (b) and Intermediate Monocytes (c) in the three groups studied (healthy controls in green dots, RA controls in grey squares and jakinib patients in beige rhombuses).
The whiskers represent the median, first and third quartile. P values are represented as follows: * P <.05, ** P <.01, ***P <.001, ****P<.0001. NS: not significant differences found.
Acknowledgements: NIL.
Disclosure of Interests: Juan José Fernández Cabero: None declared, Carmen Lasa-Teja: None declared, Alejandra Comins-Boo: None declared, David San Segundo: None declared, Marcos López Hoyos: None declared, Ricardo Blanco Pfizer, Roche, Bristol-Myers, Lilly, Galapagos, Novartis, Janssen, GSK, and MSD.