fetching data ... 
Background: Glucocorticoids (GCs) play a pivotal role in the management of inflammatory rheumatic conditions but they can adversely impact on patients in different ways. Conversely, there are certain patient characteristics that may be correlated with a poorer health-related quality of life (HRQoL).
Objectives: The objective of this study was to identify socio-demographic and clinical factors associated with HRQoL in patients undertaking GCs for a rheumatic disease.
Methods: This was a cross-sectional study using online survey methods. Participants taking GCs for a rheumatic disease from Australia/New Zealand (AU/NZ), United Kingdom (UK) and the United States of America (USA) were included. HRQoL was measured using the generic EuroQoL (EQ-5D-5L) converted into a linear EQ5D index value. Eight explanatory factors (age, sex, country, educational level, employment status, disease group, self-reported disease state, and dose of GCs) were tested for potential association with HRQoL using univariable and multivariable (hierarchical) analyses. Factors found to have a significant association with EQ5D index at a p <0.05 level in the multivariable model were considered independently associated with HRQoL.
Results: A total of 945 patients completed the EQ-5D-5L with no missing values: UK n=742 (79%), USA n=139 (15%), AU/NZ n=64 (7%); mean age was 57.6 (SD=13.6); 833 (88%) were women. Participants with self-reported active disease were 726 (77%). Those with inflammatory arthritis were 197 (21%), connective tissue disease and/or vasculitis were 402 (43%), giant cell arteritis and/or polymyalgia rheumatica were 346 (36%).
Mean (SD) EQ5D index was 0.64 (0.25); There were significant differences between groups in age (median split, t=-3.77, p <0.001); sex (t=3.40, p <0.01); educational level (F[3]=10.51, p <0.001); employment status (F[6]=37.67, p <0.001); disease group (T[2]=20.23, p <0.001); disease state (T=-8.46, p <0.001); and the dose of GCs (T=2.95, p <0.001). Worse HRQoL was associated with older age, being female, low educational attainment, being unemployed, having an inflammatory arthritis or a CTD, disease being active, and taking a higher dose of GCs. Five factors were identified as being independently associated with worse HRQoL: disease state (β=0.12, p <0.001), disease group (β=0.06, p <0.001), employment status (β =0.05, p <0.001), sex (β =0.05, p <0.001), and educational level (β =0.04, p <0.001).
EQ-5D-5L frequencies in the 3 disease categories, reported by dimensions dichotomised into no problem or any problems.
| IA (n=197) (%) | CTD/vasculitis
| GCA/PMR
| Chi-Square
|
||
|---|---|---|---|---|---|
| Mobility | No problem | 18 (9.2) | 109 (27.1) | 101 (29.2) | 30.987 (<0.001) |
| Any problems | 179 (90.9) | 293 (72.9) | 245 (70.8) | ||
| Self-care | No problem | 57 (28.9) | 220 (54.7) | 232 (67.1) | 73.604 (<0.001) |
| Any problems | 140 (71.1) | 182 (45.3) | 114 (32.9) | ||
| Activity | No problem | 17 (8.7) | 59 (14.7) | 65 (18.8) | 10.234 (0.006) |
| Any problems | 180 (91.4) | 343 (85.3) | 281 (81.2) | ||
| Pain/Discomfort | No problem | 6 (3.1) | 48 (11.9) | 27 (7.8) | 13.833 (<0.001) |
| Any problems | 191 (97.0) | 353 (87.8) | 319 (92.2) | ||
| Anxiety/Depression | No problem | 54 (27.4) | 89 (22.1) | 120 (34.7) | 14.587 (<0.001) |
| Any problems | 143 (72.6) | 313 (77.9) | 226 (65.3) |
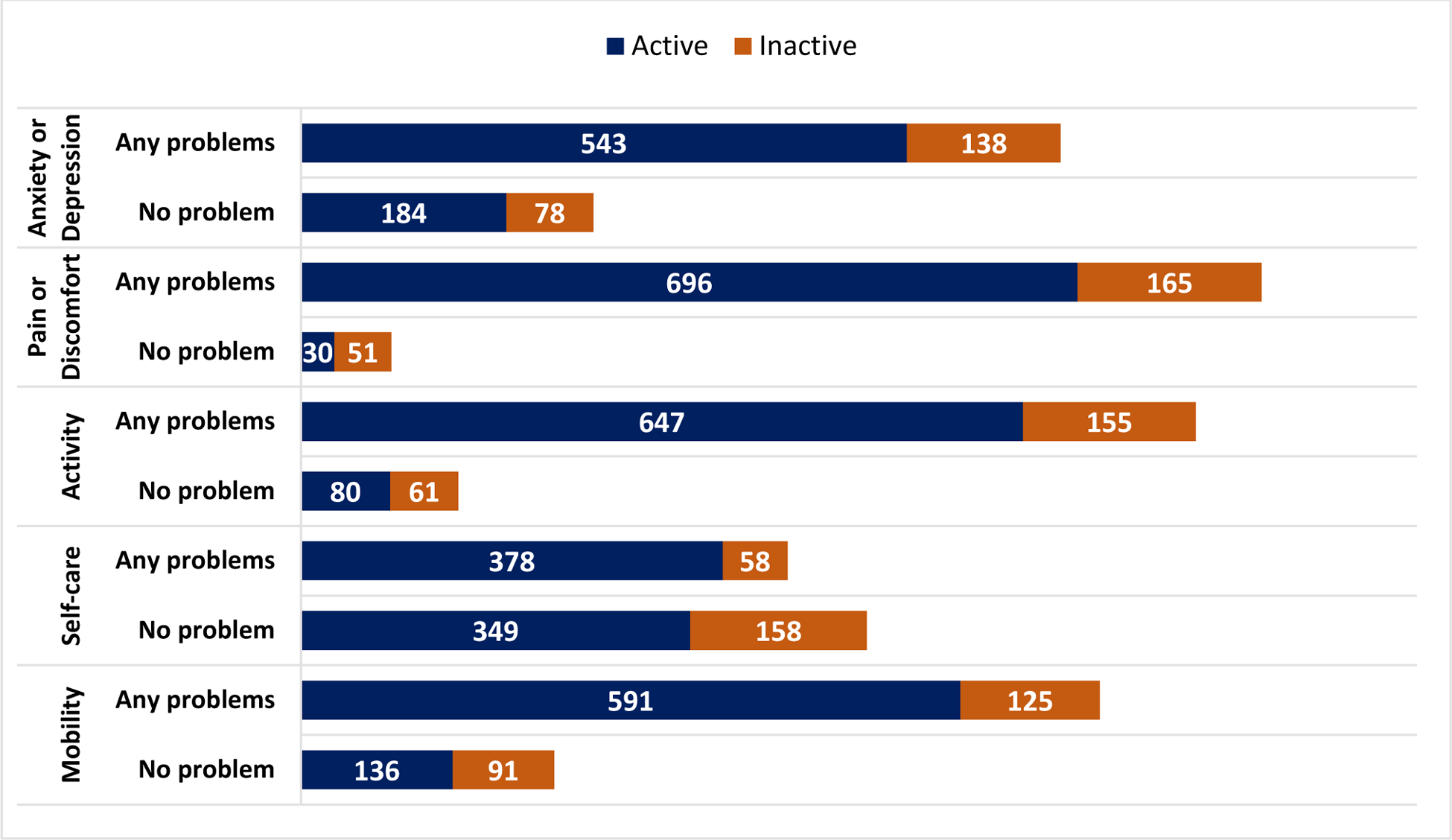
EQ-5D-5L proportions reported by dimensions dichotomised into no problem or any problems. Disease activity was patient‘s self-report of active or inactive disease.
Conclusion: We identified 5 factors which were independently associated with worse HRQoL in patients being treated with GCs. Over 80% of the variance was not explained by our model likely due to use of a generic HRQoL measure (EQ-5D-5L) as outcome, and the small number of explanatory factors tested within this survey. Further research is required to identify potential targets to support interventions.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.