fetching data ... 
Background: Physical function, as determined on a patient self-report questionnaire, is a key indicator of status in patients with rheumatoid arthritis (RA), and the most significant RA core dataset measure to predict to predict severe clinical outcomes of work disability, costs, joint replacement surgery, and premature mortality. Nonetheless, many rheumatologists do not collect a patient self-report questionnaire in routine care, and treatment is guided by quantitative measures of lesser prognostic significance, primarily laboratory tests often as the only quantitative data in a patient’s electronic medical record (EMR). Electronic formats of patient questionnaires have been developed, but implementation is difficult in many settings. An electronic version of a multidimensional health assessment questionnaire (MDHAQ) can be completed securely on mobile devices such as a patient’s iPhone or android device and conveys a secure report of quantitative scores and indices to the physician. This report is available for integration into an electronic medical record (EMR), although requiring collaboration with the EMR vendor for implementation, enabling bi-directional data exchange with EMR, integrating laboratory tests, prescription information and other relevant clinical data with MDHAQ scores.
Objectives: To recognize the potential value of an MDHAQ on a mobile device for a patient and report of quantitative MDHAQ scores and indices for a an EMR encounter note for a physcian in routine rheumatology care.
Methods: At one rheumatology setting, an MDHAQ is completed by all patients with all diagnoses at all visits. A secure website, “myprivatemed.com,” provides an electronic MDHAQ on a patient’s iPhone or android mobile phone. After completion by the patient, a report of MDHAQ scores and indices is generated for the physician without any need for scoring and/or data entry, analogous to a report of laboratory tests. The automated report provides MDHAQ scores and four MDHAQ indices, RAPID3 (routine assessment of patient index data) to assess overall clinical status in any rheumatic disease, MAS2 (MDHAQ anxiety screening index), MDS2 (MDHAQ depression screening index) and FAST4 (fibromyalgia assessment screening tool and max). Serial flowsheets of MDHAQ scores and indices depict clinical status over long periods, which may include laboratory tests and medication data if integrated into the EMR.
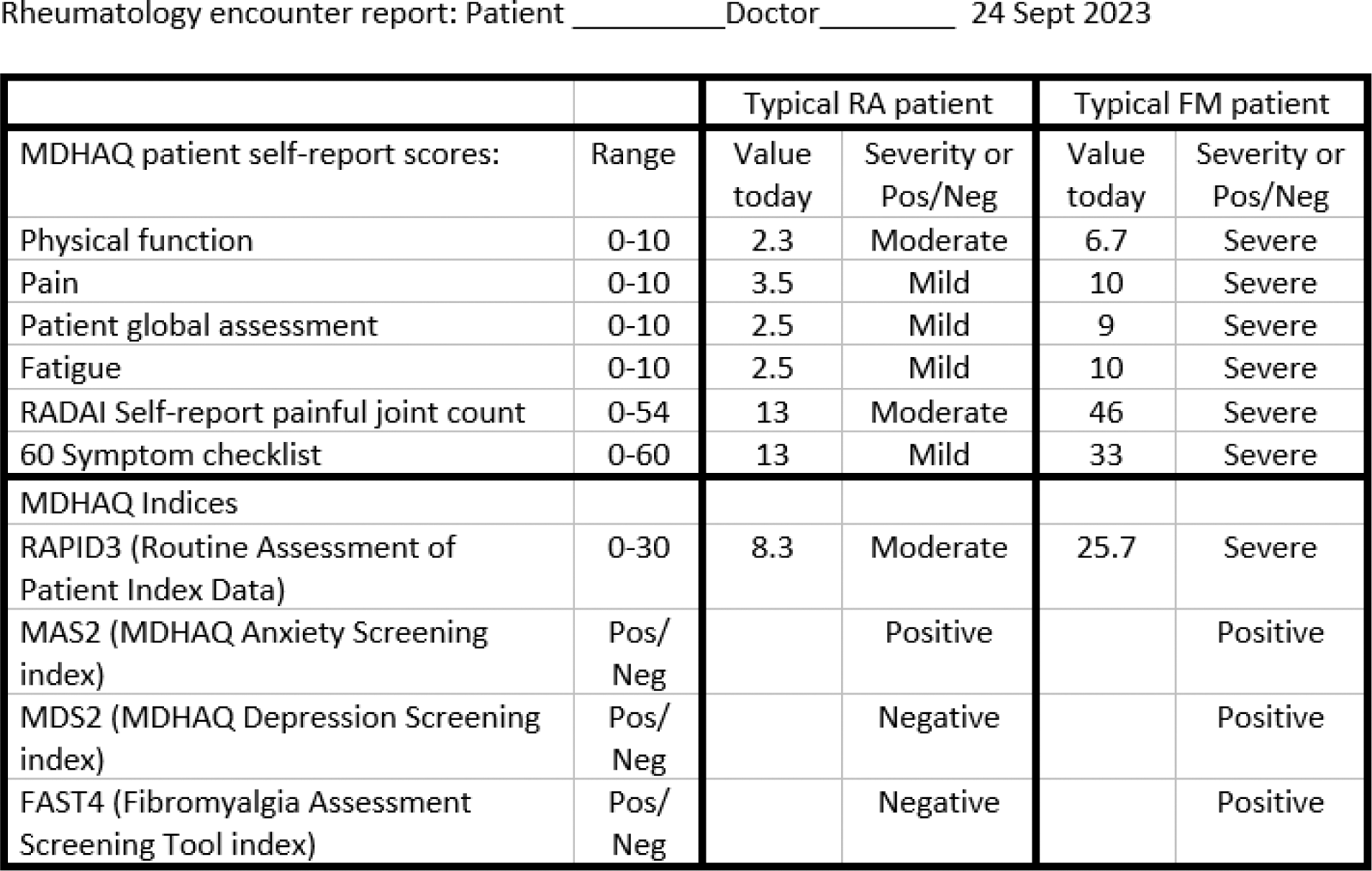
Results: The automated report for a typical RA patient indicated MDHAQ scores 2.3/10 for physical function, 3.5/10 for pain 2.5/10 for patient global assessment, 2.5/10 for fatigue, 13/54 on a RADAI (rheumatoid arthritis disease activity index) self-report painful joint count, and 13/60 symptoms on a 60-symptom checklist (Table 1). Corresponding scores for a typical fibromyalgia patient were 6.7/10, 10/10, 9/10, 10/10, 9/54, and 33/60, respectively (Table 1). Among MDHAQ indices, RAPID3 was 8.3 in the typical RA patient and 25.7 in the typical FM patient, MAS2 (MDHAQ anxiety screen) was positive in both the RA and FM patients, MDS2 (MDHAQ depression screen) and FAST4 (fibromyalgia assessment screening tool) were both negative in the RA patient and positive in the FM patient (Table 1). Serial flowsheets of scores are available for each individual patient which can be entered into an EMR through “cut-and-paste” or with collaboration of the EMR through on a secure application programming interface (API) (data not shown).
Conclusion: The mobile-enabled MDHAQ provides an effective tool for patient data collection, with seamless potential integration into EMR systems, enabling a bi-directional flow of information. Implementation of this system, although requiring collaboration with EMR vendors, offers significant potential to improve the management and clinical decision-making process in rheumatology care.
REFERENCES: NIL.
Table 1.
Acknowledgements: NIL.
Disclosure of Interests: None declared.