fetching data ... 
Background: Chondrocalcinosis is a frequently encountered pathology in rheumatology that can mimic or interfere with other diseases such as rheumatoid arthritis. As indicated in the recently established ACR/EULAR classification criteria, radiographic calcium pyrophosphate deposition (CPPD) affects the triangular fibrocartilage complex (TFCC) but also 2nd and 3rd metacarpophalangeal joints (MCP-2, MCP-3) and the carpometacarpal joint.
Objectives: We aimed to develop a deep learning approach for automatically and reliably detecting CPPD on hand radiographs, focusing on the TFCC and MCP-2, MCP-3 in a combined (according ACR/EULAR classification criteria) or separate models.
Methods: Two radiologists independently labeled a dataset of 926 hand radiographs, yielding 319 CPPD positive and 607 CPPD negative cases across the three sites of interest. CPPD presence was then predicted using a convolutional neural network. The model performance was assessed using the area under the receiver operating characteristic (AUROC) and area under the precision-recall (AUPR) curves, with heatmaps Grad-CAM) aiding in case discrimination.
Results: The algorithm for combined TFCC, MCP-2, and MCP-3 classification showed the most robust performance with a mean AUROC of 0.85 and AUPR of 0.74, a sensitivity of 0.86, a specificity of 0.72, and a precision of 0.62. The TFCC-alone model had a mean AUROC of 0.83 with a lower mean AUPR of 0.69. In contrast, the MCP-2-alone and MCP-3-alone models exhibited mean AUROCs of 0.78-0.82, but lower mean AUPRs of 0.29-0.35. Heatmap analysis revealed activation in the regions of interest for positive cases (true and false positives), but unexpected highlights were encountered possibly due to correlated features in different hand regions.
Conclusion: This study highlights the potential of an automated model for CPPD detection on hand radiographs with a high performance in the combined and TFCC-alone models. The algorithm could, for example, be used to screen larger databases or Electronic Medical Records for CPPD cases. Future work includes dataset expansion, threshold optimization, preprocessing refinement, and validation with an external dataset.
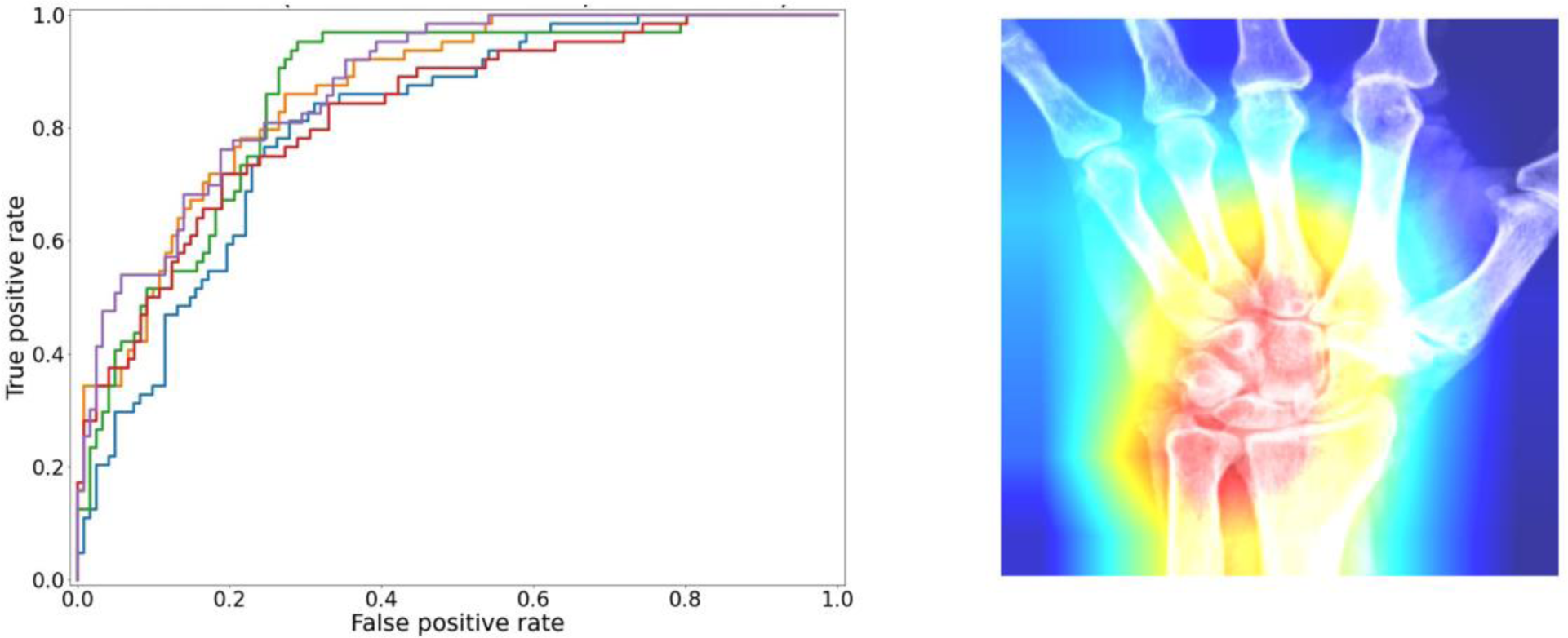
ROC curves (5-fold cross validation) for the combined TFCC, MCP-2 and MCP-3 model for the detection of CPPD on hand radiographs (on the left). The mean AUROC is 0.85 with a standard deviation of 0.02. An interpretability plot (heatmap) for combined model is shown on the right (TFCC positive; MCP-2 and MCP-3 negative).
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: Thomas Hügle Roche, Novartis, BMS, GSK, Janssen, Galapagos, Atreon, Vtuls, Elisabeth Rosoux: None declared, Tobias Manigold: None declared, Guillaume Fahrni: None declared, Deborah Markham: None declared, Fabio Becce: None declared.