fetching data ... 
Background: We recently reported that 2.7% of rheumatoid arthritis (RA) cases were polyrefractory (failure/tolerance of all b/tsDMARD classes). However, 40% of D2T-RA patients including polyrefractory RA (PFRA), lacked objective joint inflammation signs on ultrasound (US)- termed non-inflammatory refractory RA (NIRRA) whilst the remaining cases had US determined persistent inflammatory refractory RA (PIRRA). [1] EULAR suggests that rapid radiographic progression (radiographic progression above 5 units per year according to the modified Sharp/van Der Heijde scoring system) may be useful for defining D2T-RA.
Objectives: We audited the use of x-rays for potential added value in D2T-RA to PFRA.
Methods: Radiographic progression was evaluated at 2 timepoints in EULAR defined D2T RA and compared to PFRA group (failed 4 or 5 therapies depending on autoantibody status). Both hands and feet images were scored using the modified Sharp/van Der Heijde scoring system blinded to the time of radiography. Annual radiographic progression was compared between PIRRA (PDUS+) and NIRRA (PDUS-) subgroups. Annual CRP levels were calculated using the area under the curve method and furthermore annualized due to heterogeneous follow-up periods to capture the cumulative burden of inflammation.
Results: Of 247 D2T-RA patients, 102 had hands radiographs at two timepoints (mean age (SD): 60.6 (13) years, mean disease duration: 190.4 month (SD 55.7) and F/M rate n: 83/19) and 67 of these 102 patients had both hands and feet radiographs. 102 patients with an interval of mean (SD): 107.1 (48.4) months between two x-rays, a seropositivity (RF or ACPA+) rate of 76.5% (n=78) and a PFRA rate of 39.2% (n=40) were included in the final analysis. The mean annual hands radiographic progression rate for the D2T-RA population was 2.2 (SD 2.67) units and mean annual feet radiographic progression rate was 0.7 (SD 0.98). Of the 67 patients with both hands/ feet radiographs, 15 (22.4%) had rapid progression rate defined in the EULAR D2T-RA. No difference between progression in the PFRA versus other D2T patients existed.
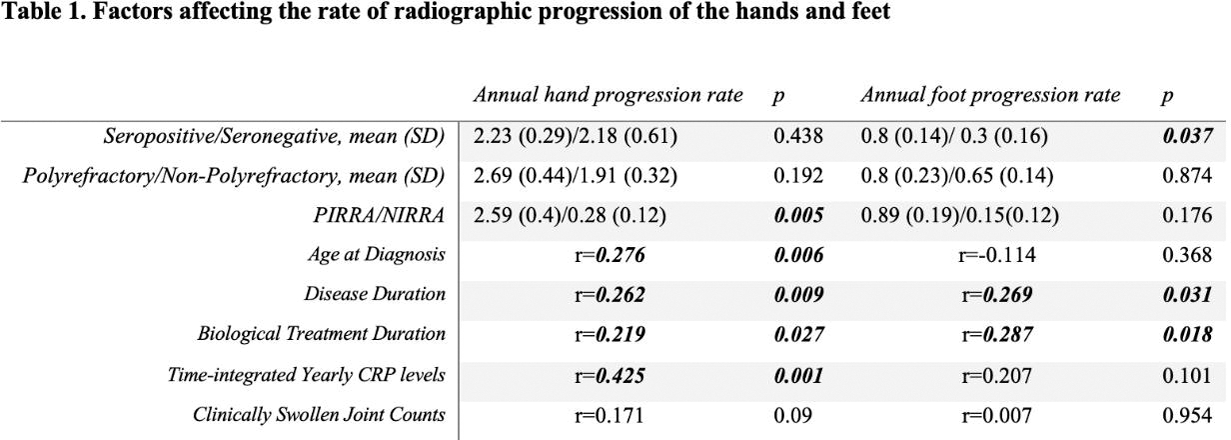
The US determined PIRRA/NIRRA ratio as 54 (88.5%)/7 (11.5%) in patients with clinically swollen joints, and the rate of hands radiographic progression in PIRRA patients was statistically significantly higher than in NIRRA patients. (p=0.005) (Table 1). In correlation analysis, time-integrated yearly CRP level was correlated with the annual hand radiographic progression rate (r=0.425, p<0.001) (Table 1). No statistically significant correlation was found between the number of clinically swollen joints and the progression rate of either the hands or the feet (Table 1).
Conclusion: This study assessed which clinical factors, including ultrasound findings, were associated with radiographic progression in D2T and PFRA patients. The radiographic progression rates in D2T to PFRA are low in the majority of RA cases and don’t differ between groups suggesting not intrinsically more destructive phenotype in PFRA. Time integrated yearly CRP levels were the best predictor of radiographic progression. Classifying as PIRRA subgroup on PDUS in patients with clinically SJC also associated with radiographic progression. In D2T-RA patients, low CRP levels and lack of PD on US may predict a lower rate of radiographic progression, even with refractory disease.
REFERENCES: [1] David P, Di Matteo A, Hen O, Dass S, Marzo-Ortega H, Wakefield RJ, Bissell LA, Nam J, Mankia K, Emery P, Saleem B, McGonagle D. Poly-refractory Rheumatoid Arthritis: An Uncommon Subset of Difficult to Treat Disease with Distinct Inflammatory and Non-inflammatory Phenotypes. Arthritis Rheumatol. 2023 Dec 7. doi: 10.1002/art.42767. Epub ahead of print. PMID: 38059326.
Acknowledgements: NIL.
Disclosure of Interests: Kerem Abacar Amgen Partner Fellowship Program, Andrea Di Matteo: None declared, Paula David: None declared, Shouvik Dass: None declared, Paul Emery Abbvie, Gilead, Lilly and Novartis, AbbVie, BMS, Lilly and Samsung, BMS, AbbVie, MSD, Pfizer, Novartis and Roche, Benazir Saleem: None declared, Dennis McGonagle Janssen, Novartis, Lilly, Pfizer, UCB, Celgene, BMS, Janssen, Novartis, Lilly, Pfizer, UCB, Celgene, BMS, Janssen, Novartis, Lilly, Pfizer, UCB, Celgene, BMS.