fetching data ... 
Background: Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by inflammatory synovitis that triggers articular cartilage destruction and bone erosion [1]. Aberrant number and/or dysfunction of regulatory T (Treg) cells may lead to many autoimmune diseases including RA [2]. Generally, Treg cells are divided into two types according to their origin: natural Treg (nTreg) cells originating from the thymus and induced Treg (iTreg) cells that develop in the periphery or in vitro [2, 3]. Nevertheless, existing studies know little about the abnormalities of Treg cell subsets in RA patients.
Objectives: This study compared the absolute number of lymphocyte, CD4 + T and Treg cell subsets in the peripheral blood of RA patients with different disease activity and healthy controls (HCs). We aimed to elucidate the significance of nTreg and iTreg cells in the development of RA, and provide a basis for further exploration of its precise treatment.
Methods: The study involved 118 RA patients hospitalized at the Second Hospital of Shanxi Medical University, which divided into three groups: 25 patients in the disease remission group (Re-RA) (DAS28 ≤ 2.6), 63 patients in the low-moderate disease activity group (L-MA-RA) (2.6 < DAS28 ≤ 5.1) and 30 patients in the high disease activity group (HA-RA) (DAS28 > 5.1), and 60 age- and gender-matched HCs. Flow cytometry were utilized to detect the level of peripheral lymphocyte, CD4 + T and Treg cell subsets.
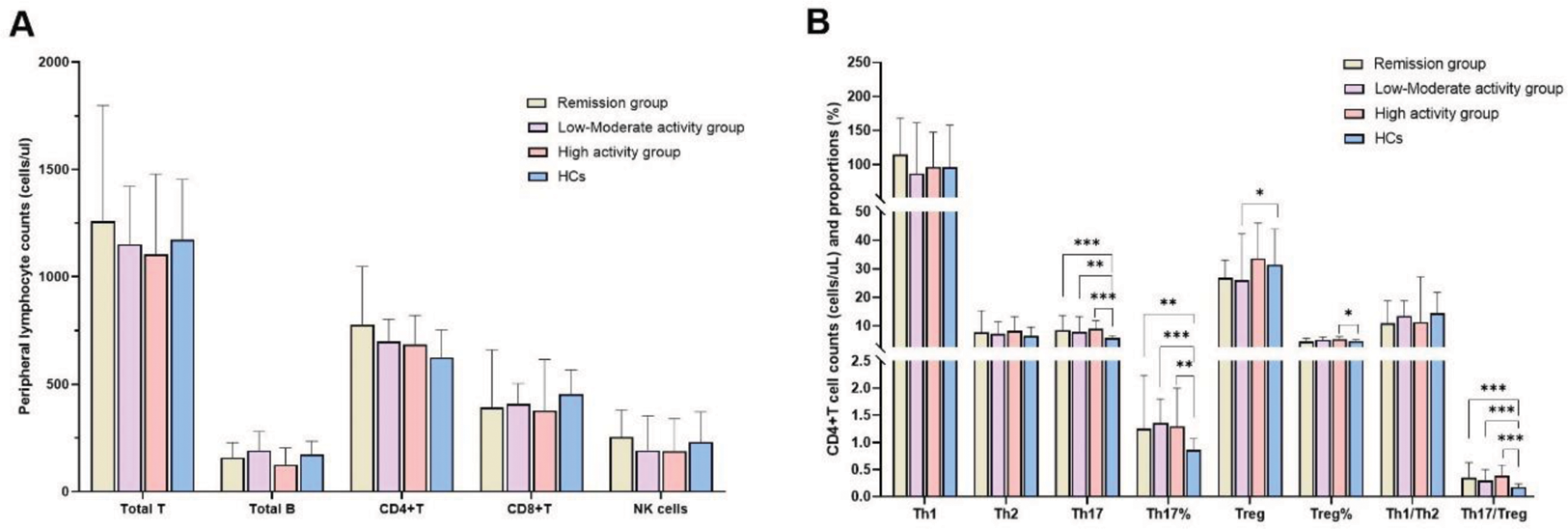
There was no significant difference in the absolute number of T, B, NK, CD4 + T or CD8 + T cells among the Re-RA, L-MA-RA, HA-RA patients and HCs.
For the comparison of CD4 + T cell subsets among three RA groups and HCs, RA patients and HCs had no significant difference in Th1 cells and Th1/ Th2 ratio. Percentage and absolute counts of Th17 cells and Th17/Treg ratios were elevated in Re-RA, L-MA-RA and HA-RA patients compared with HCs, but there was no significant difference in percentage and absolute counts of Th17 cells among the three RA groups. Moreover, absolute counts of Treg cells were lower in L-MA-RA patients than in HCs, whereas the percentage of Treg cells was higher in HA-RA patients than in HCs.
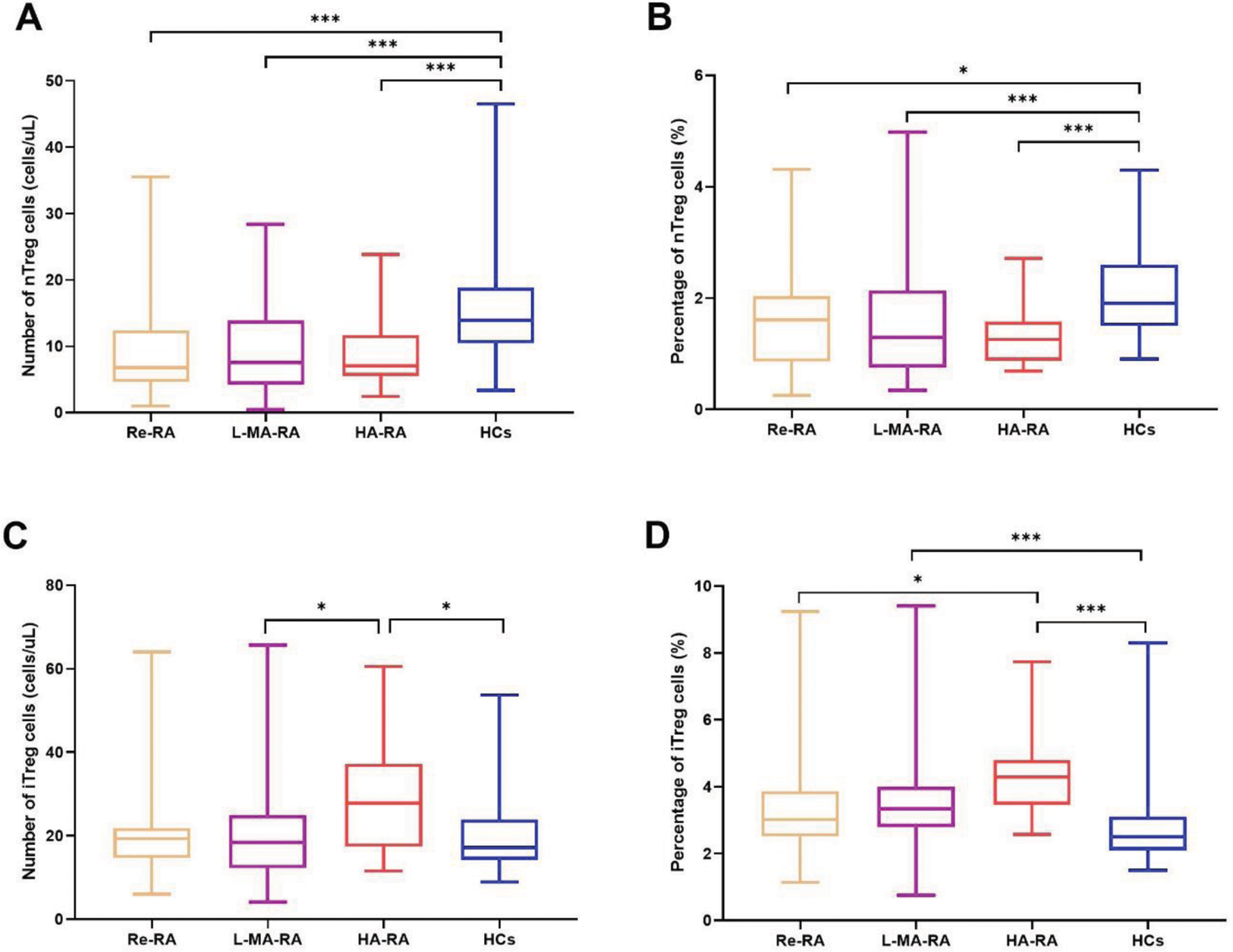
In the comparison of Treg cell subsets among three RA groups and HCs, the percentage and absolute counts of nTreg cells were decreased in Re-RA, L-MA-RA, and HA-RA patients compared with HCs, yet there was no significant difference in nTreg cell levels among the three RA groups. However, the absolute counts of iTreg cells were higher in HA-RA patients than in L-MA-RA and HCs; the percentage of iTreg cells was higher in HA-RA patients than in Re-RA and HCs, and the percentage of iTreg cells was higher in L-MA-RA patients than in HCs.
Conclusion: Our results indicated that there was difference in the levels of nTreg and iTreg cells in the peripheral blood of RA patients with different levels of disease activity. iTreg cell levels increased with disease activity of RA increased, whereas there were no similar changes in nTreg cell levels. Thus, targeted modulation of the levels of Treg cell subsets may be an effective way to promote RA remission and halt disease progression.
REFERENCES: [1] Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet 2016;388:2023-38.
[2] Yang S, Zhang X, Chen J, Dang J, Liang R, Zeng D , et al. Induced, but not natural, regulatory T cells retain phenotype and function following exposure to inflamed synovial fibroblasts. Science advances 2020;6.
[3] Zhang H, Xia N, Tang T, Nie S, Zha L, Zhang M , et al. Cholesterol suppresses human iTreg differentiation and nTreg function through mitochondria-related mechanisms. J Transl Med 2023;21:224.
Comparison of peripheral lymphocyte and CD4+T cell subsets between RA patients with the disease remission group (n=25), low-moderate disease activity group (n=63) and high disease activity group (n=30) and healthy controls (HCs, n=60). (*p<0.05, **p<0.001, ***p<0.0001)
Comparison of percentage and absolute counts of Treg cell subsets in the peripheral blood between RA patients with the disease remission group (n=25), low-moderate disease activity group (n=63) and high disease activity group (n=30) and healthy controls (HCs, n=60). (*p<0.05, **p<0.001, ***p<0.0001)
Acknowledgements: NIL.
Disclosure of Interests: None declared.