fetching data ... 
Background: Juvenile idiopathic arthritis (JIA) is most common form of childhood rheumatic disease. Growth failure and pubertal delays are potential threat to a developing child. Understanding these dynamics are crucial for optimizing patient care and addressing growth related concerns in children.
Objectives: To assess the prevalence of endocrine dysfunction in JIA and to identify potential contributory factors like disease activity and steroid use for growth failure and sexual development.
Methods: A prospective observational study was conducted between January 2022 to January 2023 and recruited 107 children of JIA fulfilling revised International League of Associations for Rheumatology classification criteria with disease duration of more than six months, attending outpatient and inpatient facility in Department of Clinical Immunology and Rheumatology, King George’s Medical University. It excludes individuals with secondary amyloidosis, active macrophage activation syndrome or other genetic growth and sexual developmental disorders. Demographic, clinical, and anthropometric evaluation were done at baseline. Pubertal maturity was assessed by characterizing individuals Tanner stage. Disease related parameters like disease activity, damage, quality of life and functional status were assessed by Juvenile arthritis disease activity score (JADAS27), Juvenile arthritis damage index (JADI), Paediatric rheumatology quality of life questionnaire (PRQoL) and Childhood health assessment questionnaire (CHAQ), respectively. Serum growth hormone (GH), insulin like growth factor 1 (IGF 1), IGF 1 binding protein 3 (IGFBP3) were measured at baseline and expressed as an absolute value as well as standard deviation score (SDS). Serum Follicle-stimulating hormone (FSH), Luteinizing hormone (LH), Estradiol and Testosterone levels were checked. Patients were followed up for one year and growth velocity was recorded.
Results: Out of 107 JIA patients, 72 were boys (67.3%) of age 13 years (± 4 years). The age of onset was 10 years (± 4 years) with a disease duration of 33 months (± 24 months). Enthesitis related arthritis (51.4%) was the most frequent diagnosis among our study population followed by RF negative polyarthritis (15%). Baseline mean glucocorticoid intake was 2.2 (± 5.4) mg/day, with a duration of 4.6 (± 10.3) months. Average cumulative dose of glucocorticoid in our study population was 572.2 (± 1260.7) mg.
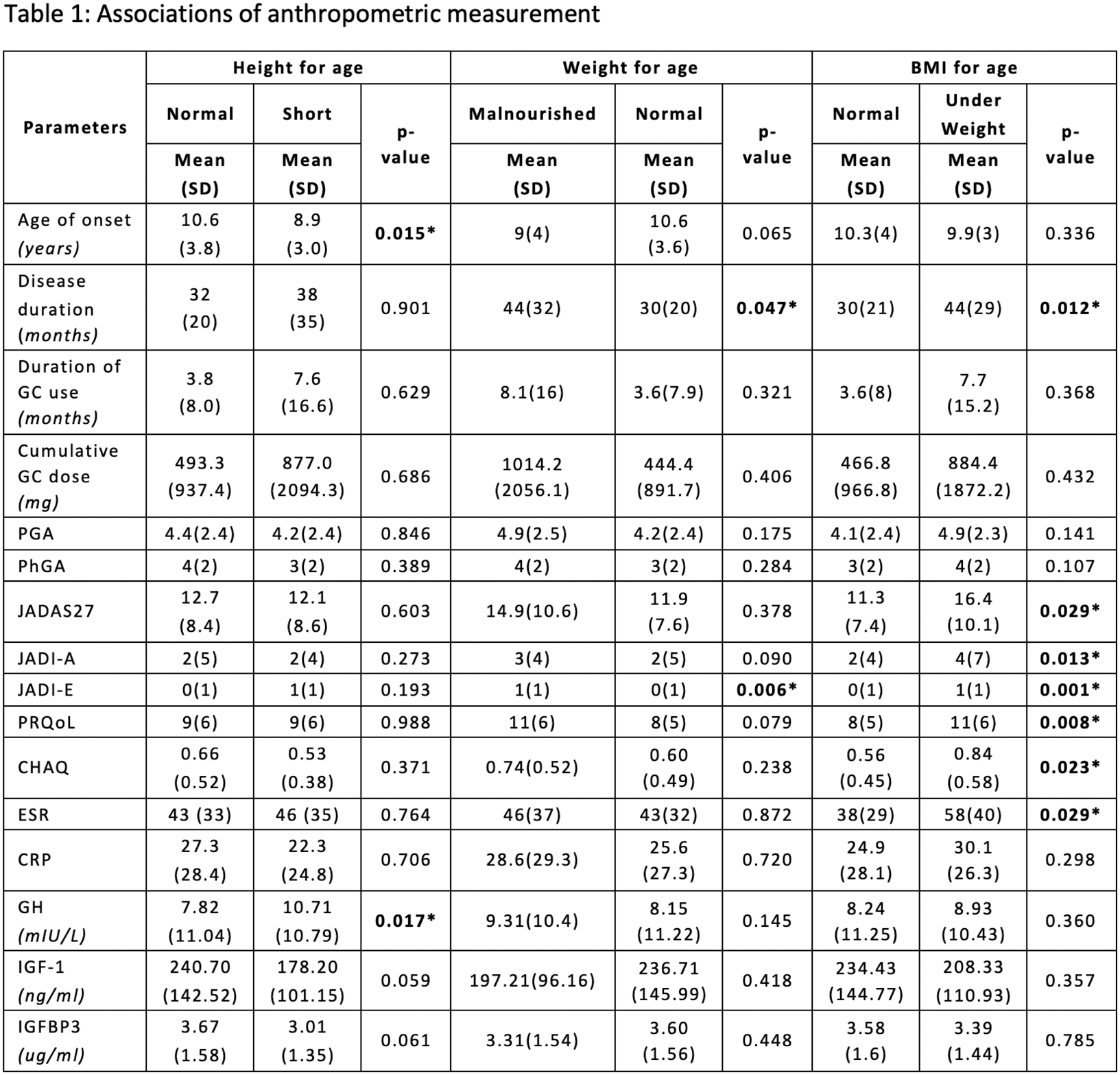
Anthropometric measurement revealed 20.6% were stunted, 22.4% were malnourished and 25.2% had low BMI for their respective age. Shorter individual were more likely to have early age of disease onset and higher GH level but less likely to have enthesitis related arthritis. Malnourished individuals had higher duration of illness and higher extra-articular damage. Changes in BMI were more robust which shows a close association with disease related factors (Table 1).
Majority of children had attained age-appropriate tanner stage (72.4%). Delayed puberty and menarche were noticed only in 2.8% of children. Most of the patients had normal gonadotrophins with low sex hormones. Low estradiol was seen in 31.4% of girls with a clear association with long term steroid use. Though 47.2% of boys had low testosterone but it didn’t reach statistical significance for any disease or therapy related factors.
Majority of the patients showed normal growth velocity for their respective age at one year follow up visit. Slower growth velocity was observed in 22.4% of children but not attributable to any of those baseline characteristics like disease activity, steroid use, or hormonal levels. Neither GH nor IGFBP3 SDS correlates well with height SDS.
Conclusion: Juvenile idiopathic arthritis is linked to clinical and subclinical endocrinal dysfunction. One-third of children with JIA experience growth failure and delayed puberty, primarily due to growth hormone resistance and alterations in the GH-IGF1 axis. Malnutrition and stunted growth should be considered during childhood arthritis treatment due to their impact on health and quality of life.
REFERENCES: NIL.
Acknowledgements: I am thankful to Prof. Wahid Ali (Department of Pathology), Prof. Mala Kumar (Department of Paediatrics), Prof. Ajai Singh (Department of Paediatric orthopaedics), and Assist. Prof. Saurabh Kumar (Department of Radiology) for their constant support and critical review.
Disclosure of Interests: None declared.