fetching data ... 
Background: SAPHO syndrome is a rare autoinflammatory disease characterized in children by chronic non-bacterial osteitis (CNO), associated to a heterogenous dermatological involvement, ranging from Palmo-plantar pustulosis (PPP), to psoriasis vulgaris (PV), acne, hidradenitis suppurativa (HS), and pyoderma gangrenosum (PG). A recent study [1] suggested the existence of two different disease clusters in pediatric SAPHO syndrome (pSAPHO) based on skin manifestations: an acne-HS-PG group (male prevalence and disease onset in puberal age with skin manifestations refractory to multiple treatments) and a PPP-PV group (female prevalence and disease onset in prepuberal age with osteoarticular manifestations).
Objectives: to confirm the presence of different disease clusters of pSAPHO in an italian multicentric cohort of patients, and to evaluate the efficacy of the different treatments in pSAPHO syndrome, compared to CNO.
Methods: SAPHO patients were enrolled in the Eurofever Registry and the data retrospectively analysed. Patients with pSAPHO were divided into an acne-HS-PG group and a PPP-PV group, and were compared to a CNO group without skin manifestations. Comparison of frequencies between groups was performed by the means of the Chi-square test or by the Fischer’s Exact test.
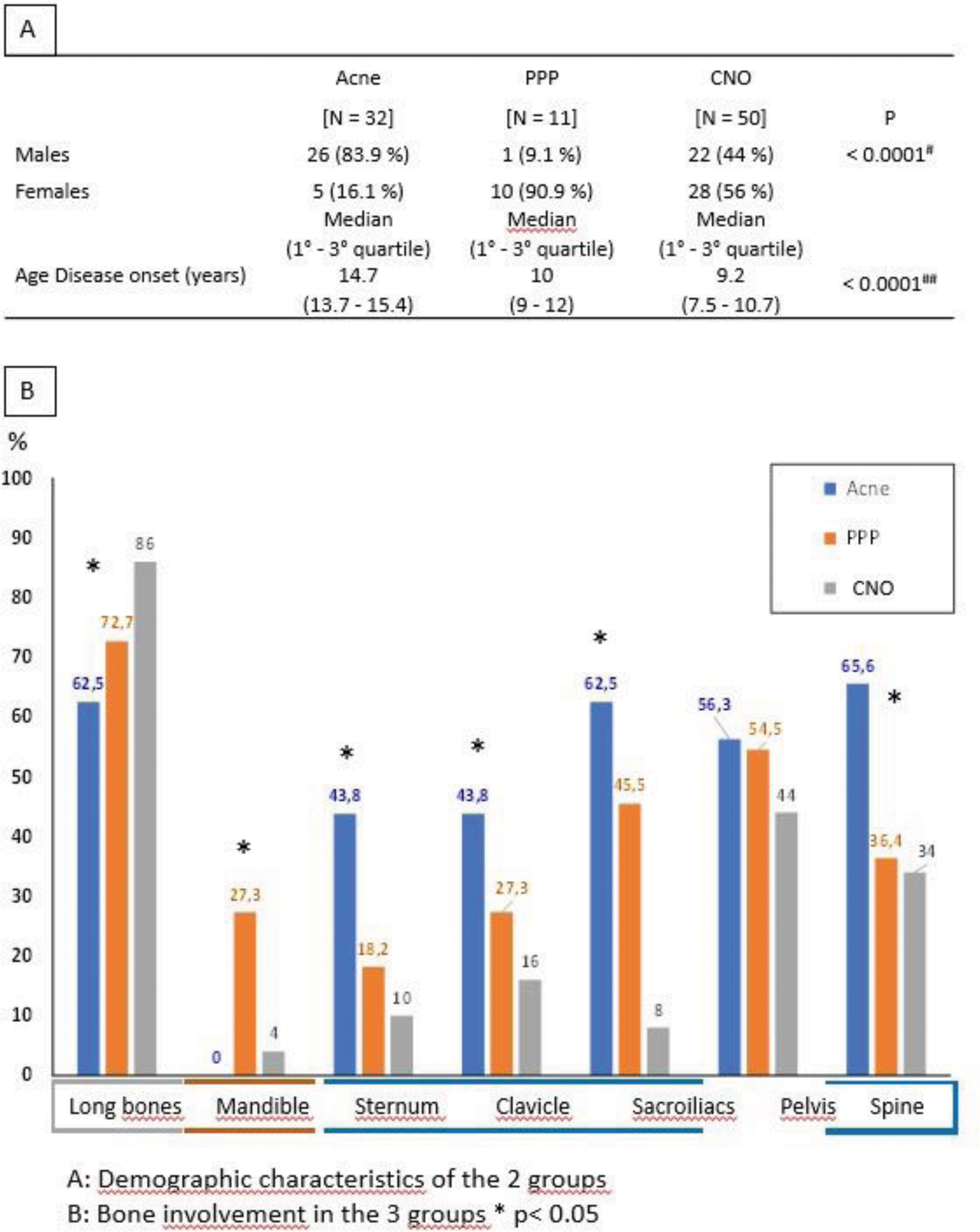
Results: 43 pSAPHO patients with skin manifestations (32 acne-HS-PG and 11 PPP-PV) were enrolled and compared to 50 CNO. In the Acne-HS-PG group, 83.9% of the patients were males, with disease onset in puberal age with skin manifestations (median 13.7 years), and the appearance of osteoarticular symptoms in the following year in 81% of patients. In the PPP-PV group, 90.9% of patients were females, with disease onset in 100% of patients with osteoarticular manifestations in prepuberal years (median 10 years), and with the appearance of skin manifestations in the following year. In the CNO group there were no gender differences, with a median age at disease onset of 9.2 years. A statistically significant difference was found between the 3 groups in terms of sex (p< 0.0001), and between acne-HS-PG and PPP-PV and acne-Hs-PG and CNO for the age at disease onset (p< 0.0001) (Figure 1A). Moreover, a different osteoarticular involvement was evident in the 3 groups: all patients showed typical metaphyseal involvement, even if it was prevalent in the CNO group (86%, p=0.04), while an axial pattern (sterno-clavicular-spine-sacroiliacs) was more frequently present in the acne-HS-PG group (p<0.01), and a mandibular involvement in the PPP-PV group (p<0.01) (Figure 1b). The 3 groups presented also a different response to treatments: in the CNO group, NSAIDs, methotrexate and salazopyrin were more frequently used (p<0.05), and were efficacious in about 40% of patients, while 36% required bisphosphonates (BP), and 28% a biologic therapy. Similarly, in the PPP-PV group 30% of patients responded to NSAIDs alone, 30% to BP while 30% required the addition of a biological therapy. The skin responded well to the topical therapies or to DMARDs. In the acne-HS-PG group instead, there was a prevalent use of systemic steroids (50% of patients, p<0.05) and biological therapies (81% of patients, p<0.05). Among these, the combination Adalimumab/methotrexate was the more efficacious, with a remission achieved in 53% of patients. The skin resulted particularly difficult to treat in all the patients and was the cause of a therapy cycling.
Conclusion: This study confirms the presence of 2 different disease clusters in pSAPHO based on the skin manifestations: an acne-HS-PG group characterized by a male predominance with puberal disease onset with skin manifestations particularly refractory to treatments, and a PPP-PV group characterized by female predominance with prepuberal disease onset with osteoarticular manifestations. These findings warrant a different therapeutical approach based on skin manifestations, and highlight the need of a new disease classification.
REFERENCES: [1] Matucci-Cerinic C, et al. Semin Arthritis Rheum. 2023 Dec;63:152277.
Acknowledgements: NIL.
Disclosure of Interests: Caterina Matucci-Cerinic: None declared, Anna Attico: None declared, Clara Malattia: None declared, Alessandro Consolaro: None declared, Silvia Rosina: None declared, Luciana Breda: None declared, Saverio La Bella: None declared, Marco Cattalini: None declared, Francesca Ricci: None declared, Giovanni Conti: None declared, Adele Civino: None declared, Francesco Licciardi: None declared, Letizia Baldini: None declared, Antonella Insalaco: None declared, Francesco La Torre: None declared, Serena Pastore: None declared, Giovanni Filocamo: None declared, Gisella Beatrice Beretta: None declared, Gabriele Simonini: None declared, edoardo marrani: None declared, Angela Pistorio: None declared, Stefano Volpi SOBI, Roberta Caorsi: None declared, Nicolino Ruperto Abbvie, Aclaris, Amgen, AstraZeneca, Aurinia, BMS, Boehringer Ingelheim, Eli Lilly, Galapagos, Guidepoint, Janssen, Novartis, Pfizer, Sanofi., Abbvie, Aclaris, Amgen, AstraZeneca, Aurinia, BMS, Boehringer Ingelheim, Eli Lilly, Galapagos, Guidepoint, Janssen, Novartis, Pfizer, Sanofi., Gianmaria Viglizzo: None declared, Marco Gattorno Novartis, SOBI.