fetching data ... 
Background: Anti-Ro52 antibodies are present in autoimmune connective tissue diseases (AICTD), as Sjögren’s syndrome (SSj), systemic lupus erythematosus (SLE), systemic sclerosis (SSc) or idiopathic inflammatory myopathies (IIM). Anti-Ro52 antibody positivity (Ro52+) has been related to more severe clinical phenotypes, including interstitial lung disease (ILD). [1] The microcirculation involvement in patients with anti-Ro52 antibodies is yet to be disclosed.
Objectives: The aim of this study is to analyze the prevalence of Ro52+ in AICTD and its association with microcirculation, organ involvement and immunologic profile.
Methods: This is a cross-sectional retrospective study, enrolling patients who underwent nailfold capillaroscopy (NFC) in an outpatient clinic, between 2020 and 2022. NFC results and electronic medical records were consulted for epidemiologic, clinical and immunological data that was later anonymized. Continuous outcomes were compared with unpaired Student t-test, Welch t-test or Mann-Whitney U test. The alpha risk was set to 5% and two-tailed tests were used. A multivariate logistic regression was performed to assess the relation between Ro52+ and NFC scleroderma pattern, sclerodactyly, lung, muscle, cardiac and esophageal involvement, Raynaud’s phenomenon (RP) and immunological profile. Heteroskedasticity and normality of residuals were assessed respectively by the White test and the Shapiro-Wilk test. A p-value of 0.05 was considered statistically significant. Patients with missing data were excluded from the analysis. To address potential biases in baseline characteristics between groups, a 1:1 propensity score matching without replacement was performed, using a logistic regression model. The common support assumption was assessed using the Kolmogorov-Smirnov nonparametric test. Common support intervals were determined using the trimming method and kernel density estimators.
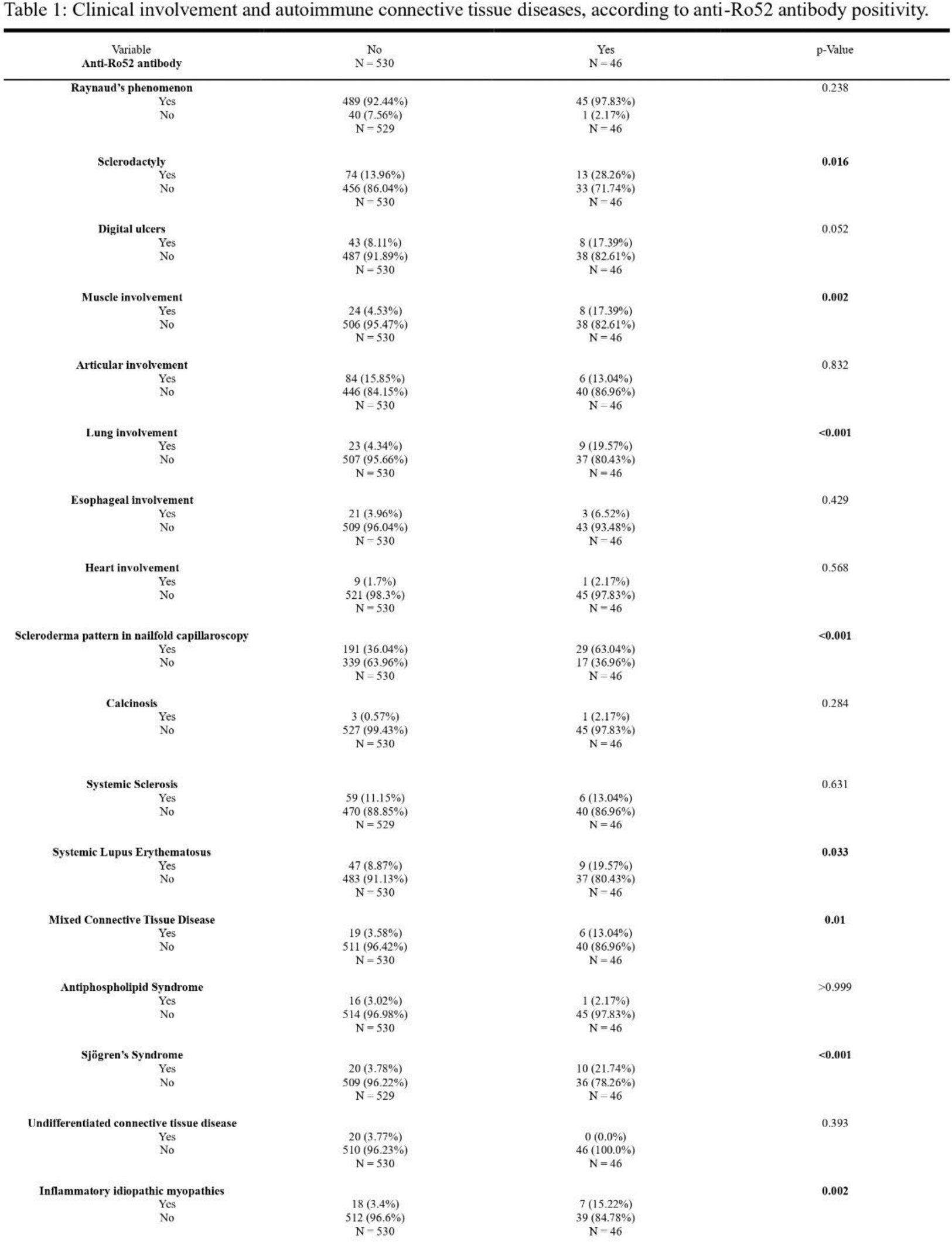
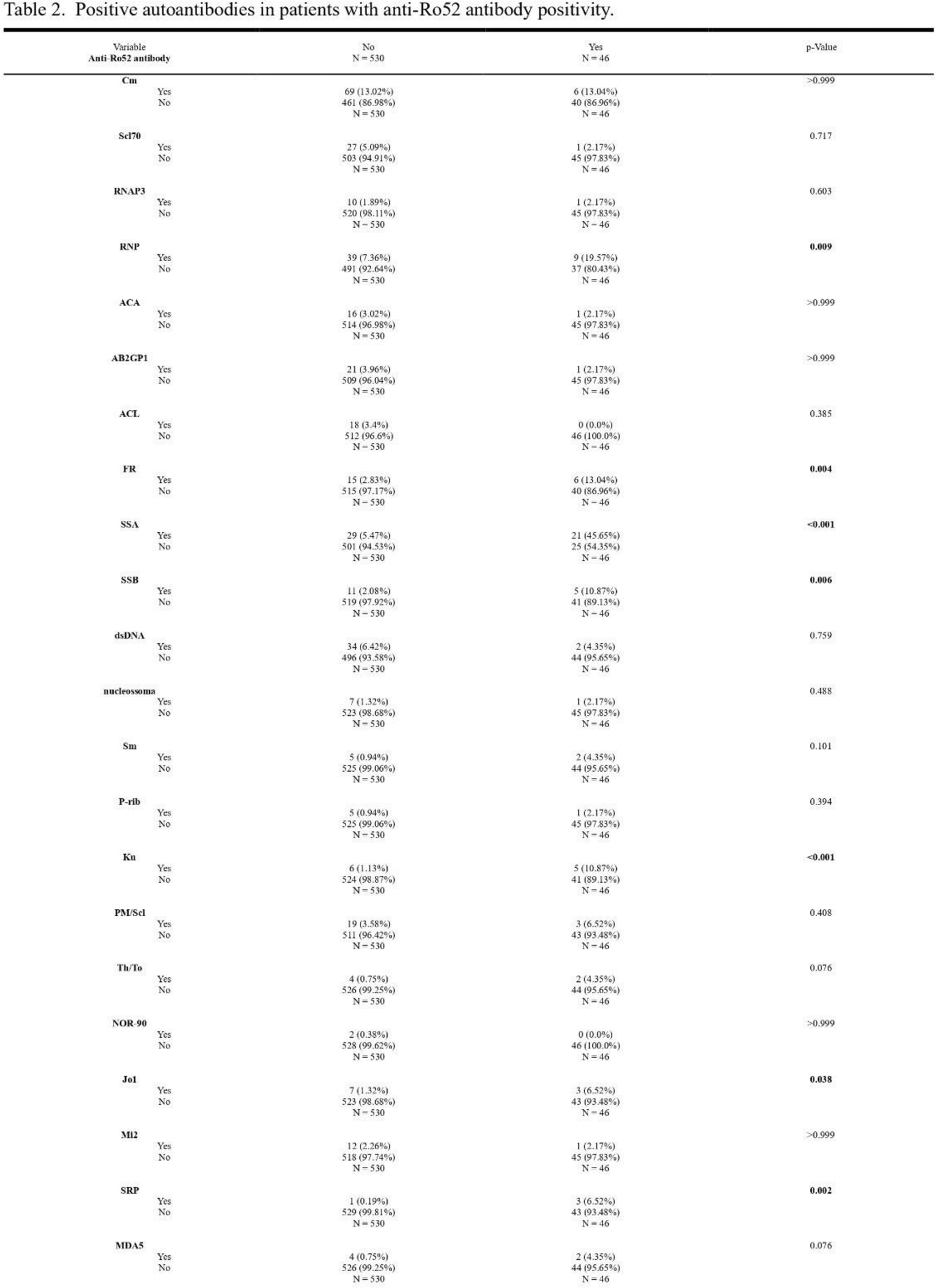
Results: NFC was performed in 643 patients during the three-year period, but only 576 had complete clinical information or available data. Of these, 84,20% were women, with mean age of 42,69 ± 19,51 years. Anti-Ro52 antibody was positive in 7,99% (n=46) - Table 1. Ro52+ patients had more frequently sclerodactyly (p=0,016), muscle (p=0,002), lung (p<0,001) and microcirculation involvement (p<0,001), the latter defined as scleroderma pattern in NFC. SLE (p=0,033), mixed connective tissue disease (p=0,01), SSj (p<0,001) and IIM (p=0,002) diagnosis were also more prevalent in this group. Correlation of immunologic markers was relevant for anti-RNP (p=0,009), anti-SSA (p<0,001), anti-SSB (p=0,006), anti-Ku (p<0,001), anti-Jo1 (p=0,038), anti-SRP (p<0,002) antibodies and rheumatoid factor (p=0,004) - Table 2. In multivariate analysis, Ro52+ was associated to higher rates of scleroderma pattern on NFC (OR=3,26, [1,44;7,38], p=0,0047), lung involvement (OR=7,46, [2,6; 21,36], p=0,0002) and sclerodactyly (OR=3,55, [1,51; 8,34], p=0,036), but not with muscle, esophageal and cardiac involvement or Raynaud’s phenomenon. Analyzing AICTD through Ro52+ matching groups, using a logistic regression model, Ro52+ was an independent predictor of scleroderma pattern (p=0,005).
Conclusion: Ro52+ is independently related to the existence of sclerodactyly, lung and microcirculation involvement. It is frequently present with other antibodies associated to AICTD, such as anti-RNP, anti-SSA, anti-SSB, anti-Ku, anti-Jo1 and anti-SRP antibodies, which could represent an epiphenomenon of a strong immune response, directly participating in tissue damage. [1] The presence of anti-Ro52 antibodies should induce clinicians to suspect overlapping AICTD syndromes and perform regular screenings of microvascular and lung involvement. Ro52+ may act as a prognostic marker in AICTD, being predictive of more severe microvascular involvement.
REFERENCES: [1] Decker P, Moulinet T, Pontille F, et al. An updated review of anti-Ro52 (TRIM21) antibodies impact in connective tissue diseases clinical management. Autoimmun Rev. 2022 Mar;21(3):103013. doi: 10.1016/j.autrev.2021.103013. Epub 2021 Dec 9. PMID: 34896652.
Acknowledgements: Virgínia Bernardino, Cristina Henriques
Disclosure of Interests: Vera Bernardino Astrazeneca, GSK, Ana Rodrigues: None declared, Melissa Fernandes: None declared, Ana Llado: None declared, Madalena Vicente: None declared, Marta Botelho de Sousa: None declared, Rita Vieira: None declared, Renata Martinho: None declared, Sara Dias: None declared, Ana Rita Gomes: None declared, Anna Taulaigo: None declared, Sara Guerreiro Castro: None declared, Eunice Patarata: None declared, Heidi Gruner: None declared.