fetching data ... 
Background: Fever of unknown origin (FUO) is defined as a condition characterized by fever (≥ 38.3°C) without explanation despite minimal standard diagnostic tests in an immunocompetent patient [1]. Inflammation of unknown origin (IUO) is defined as an illness lasting more than 3 weeks, during which the body temperature is ≤ 38.3 °C on several occasions, the inflammatory markers are elevated, and for which no diagnosis could be established, during at least 3 outpatient visits or 3 days of hospital investigation [2].
Objectives: To evaluate the usefulness of 18F-FDG PET/CT to guide the diagnosis of patients with FUO and IUO.
Methods: We identified all patients with FUO/IUO who underwent 18F-FDG PET/CT at the University Hospital of Pitié-Salpêtrière (France) between 2009 and 2022.
Inclusion criteria were i. age 16 to 70 years; ii. fever > 38°C in at least two occasions or duration of fever ≥ 3 weeks; elevated inflammatory markers (CRP>5 mg/dL).
Exclusion criteria were i. treatment by prednisone or equivalent at a dose > 10 mg/d; ii. treatment by biologic DMARDs at the time of the examination or the 10 days before.
Patients medical charts were reviewed and 18F-FDG PET/CT findings were analysed after stratification on 3 disease groups: i. patients with neoplasia, ii. patients with infections, iii. patients with immune-mediated inflammatory disorders (IMID).
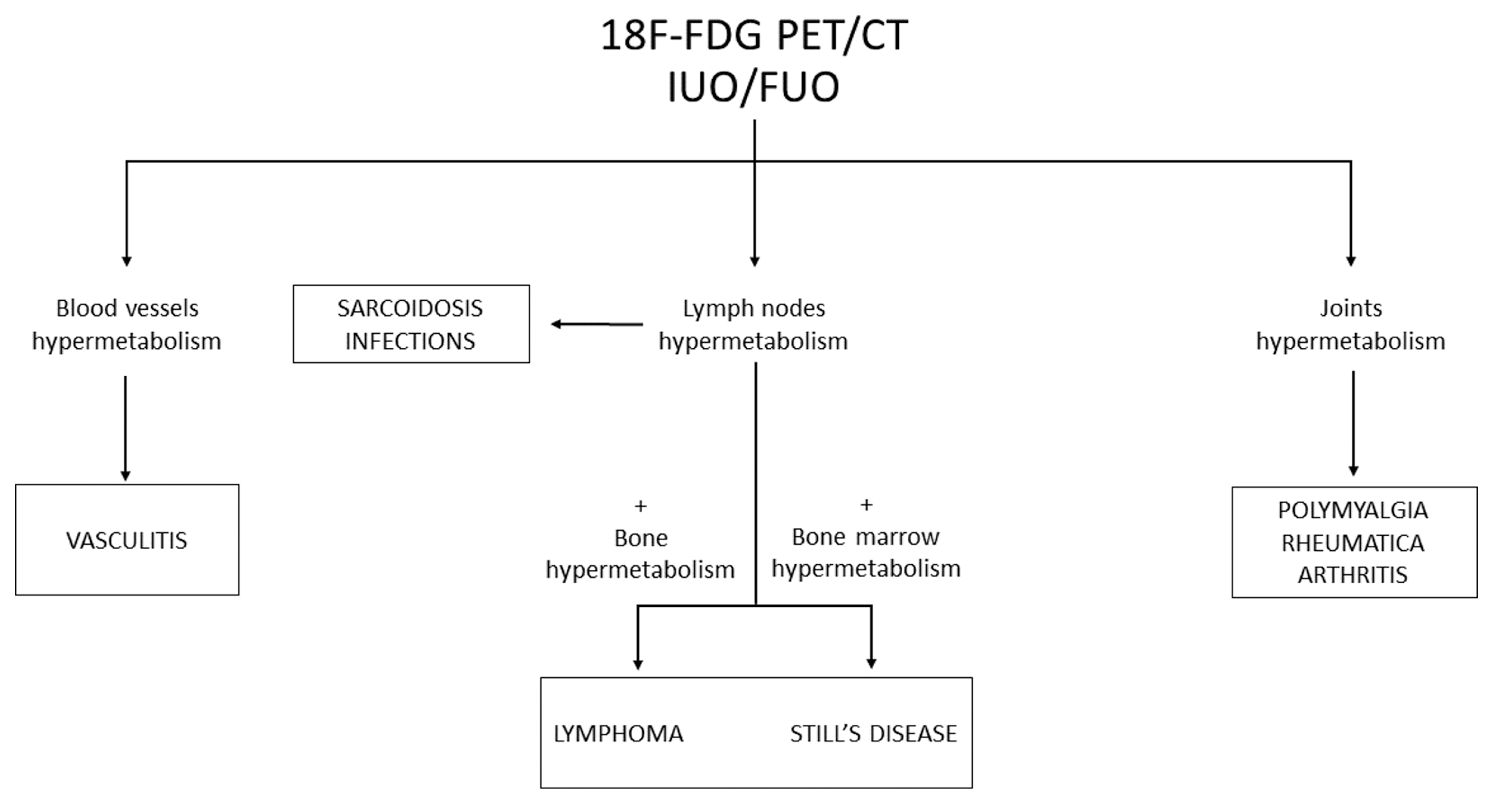
Results: We assessed 331 patients who fulfilled the inclusion/ exclusion criteria and underwent 18F-FDG PET/CT. Among those, 81 were classified as FUO whereas 250 as IUO. Among these patients, 128 (38.7%) showed findings of 18F-FDG PET/CT hypermetabolism in one or more areas. The final diagnoses of these patients were: 16 neoplasia (mainly lymphoma), 42 infections (mainly sepsis and lung infections), and 70 patients with IMID. Patients with neoplasia were characterized by a higher prevalence of hypermetabolism of lymph nodes (p=0.008), and bones (p=0.003), compared to other diagnosis groups. In infection group, 18 patients (42.90%) showed a lymph node hypermetabolism. The IMID group was the most heterogenous. Lymph nodes hypermetabolism was mainly retrieved in Still’s disease (83.33%) and sarcoidosis (100%). Furthermore, hypermetabolism of bone marrow was described in 4 patients (6.67%) with Still’s disease. Hypermetabolism of blood vessels were described in nearly all patients (85.71%) with vasculitis. In addition, findings of hypermetabolism of joints were described in patients with polymyalgia rheumatica (100%) and spondylarthritis (100%).
Conclusion: 18F-FDG PET/CT is interesting in patients with FUO/IUO to identify hypermetabolism patterns suggestive neoplasia, infections or IMID. We propose a practical diagnostic algorithm to assist clinicians in making an accurate and timely diagnosis (Figure 1).
REFERENCES: [1] Wright WF, et al. Am J Med. 2022.
[2] Vanderschueren S, et al. Eur J Intern Med. 2009.
Acknowledgements: NIL.
Disclosure of Interests: None declared.