fetching data ... 
Background: Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by joint inflammation and cartilage destruction. In addition to its impact on musculoskeletal system, RA has been recognized as a systemic disease associated with an increased risk of cardiovascular disease. Current CV risk screening and management strategies underestimate the actual CV risk in RA. Thus, an adequate CV risk stratification has special relevance in RA to identify patients at risk of CV disease.
Objectives: To evaluate the cardiovascular risk profile in patients with RA by assessing both traditional CVD risk factors, carotid ultrasound finding and risk estimation using SCORE and SCORE2.
Methods: A cross-sectional study was performed including adult moderate to severe RA patients who had initiated treatment with JAK inhibitors or anti TNF. Traditional risk factors, including age, gender, smoking status, hypertension, dyslipidemia, and diabetes were evaluated. The widely used scoring systems, such as the Systematic Coronary Risk Evaluation (SCORE) and its updated version, SCORE2, were employed to estimate the global cardiovascular risk in this population. Furthermore, carotid ultrasound examinations were conducted to investigate subclinical atherosclerosis in RA patients. Measurements of carotid intima-media thickness (IMT) were obtained as a surrogate marker of early vascular damage. Additionally, the presence of atherosclerotic plaques, a hallmark of advanced vascular disease, was documented. This study was performed from September-2022 to April-2023. The study was approved by the Ethics Committee and statistical analysis was performed using R.
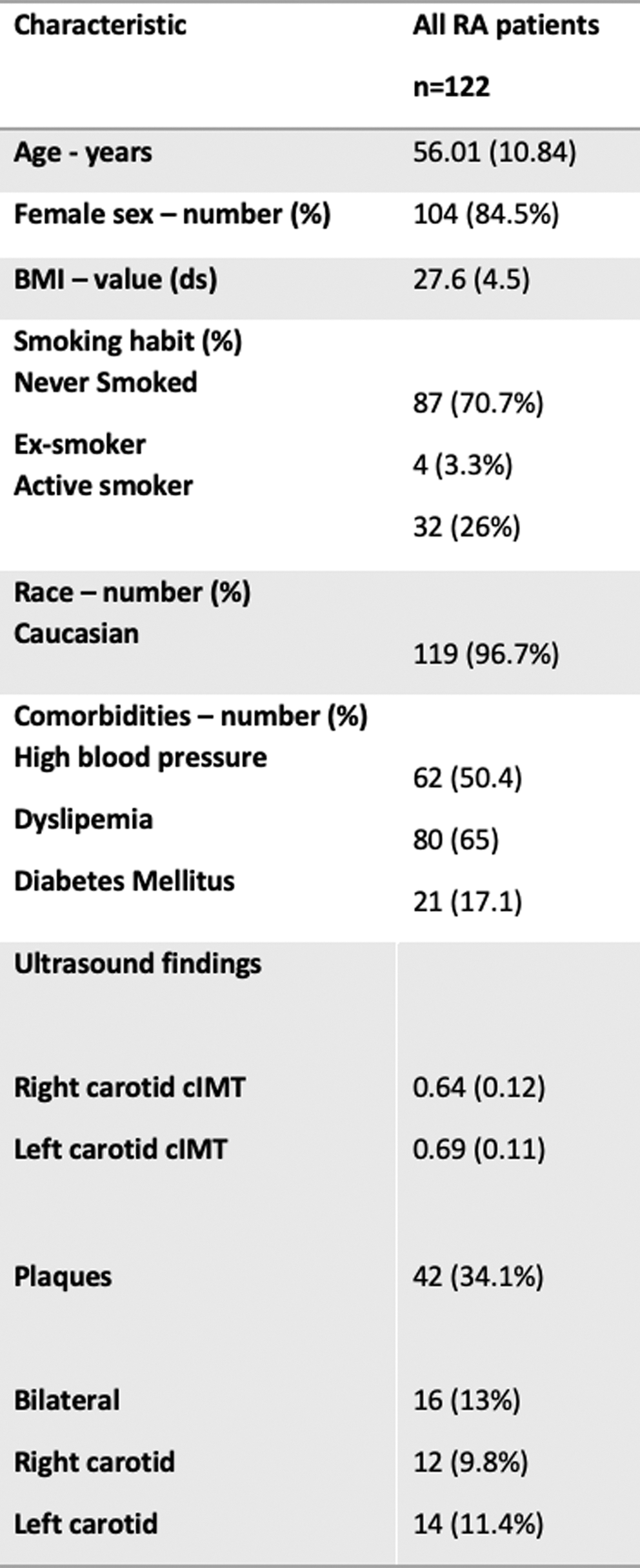
Results: A total of 122 patients were included in the study. Demographical and clinical variables are shown in Table 1. Among the RA patients, a high prevalence of CVD risk factors was observed. The mean values of SCORE and SCORE2 indicated a moderate to high estimated 10-year risk of fatal CVD events in this population (mean SCORE: 2.77%, mean SCORE2: 4.07%).
Carotid ultrasound measurements revealed an increased mean IMT in RA patients (mean right carotid cIMT: 0.64 [0.12]; mean left carotid cIMT 0.69 [0.11]). Furthermore, a substantial proportion of patients (34.1%) displayed the presence of atherosclerotic plaques.
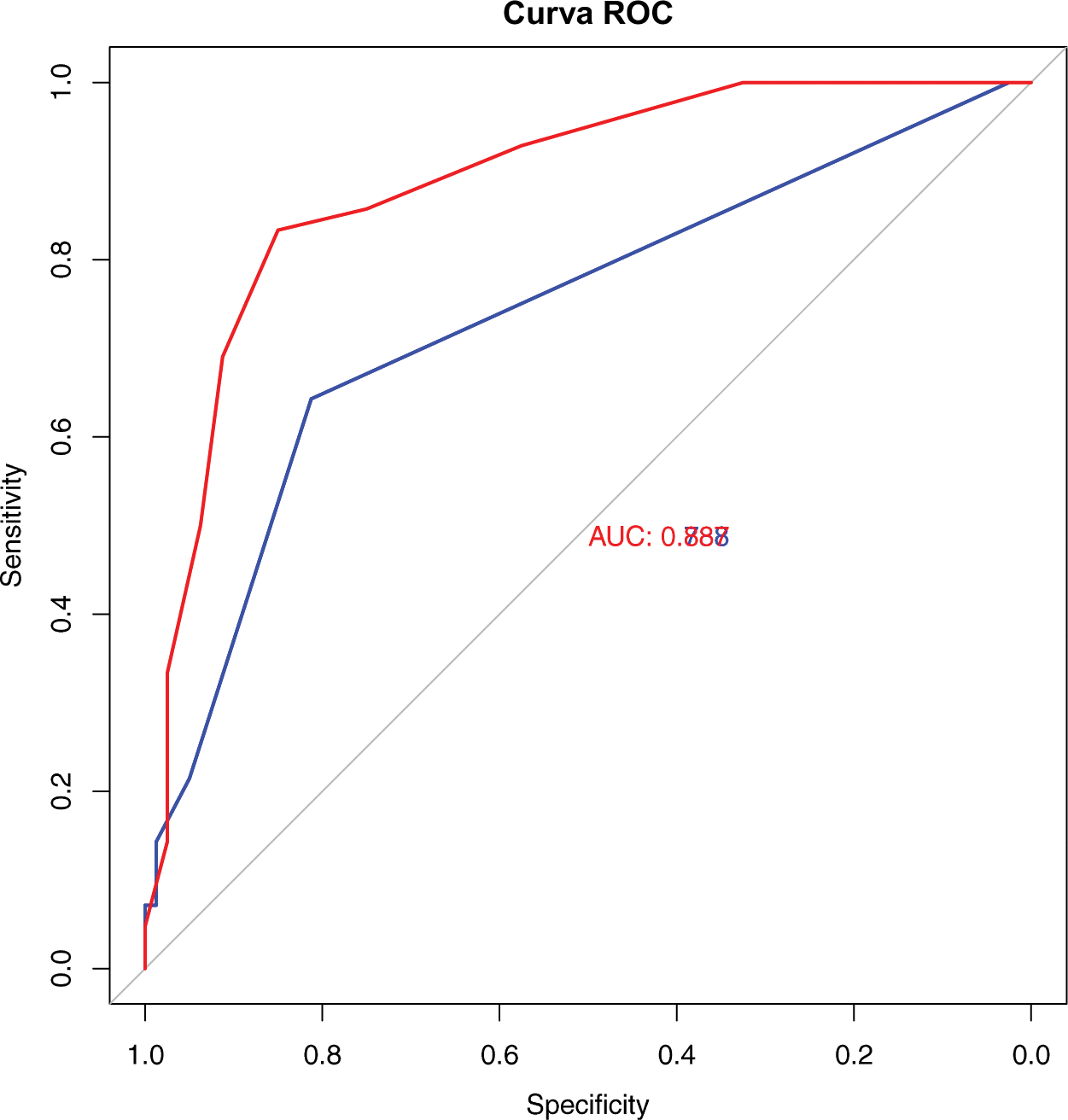
The concordance correlation coefficient between SCORE and SCORE2 demonstrated a significant moderate positive relationship (estimate 0.32 [0.19-0.43] IC 95%). ROC curves were calculated for SCORE and SCORE2 regarding their predictive capacity for plaques, showing a significant difference between them (p<0.001) indicating a superior predictive capacity of SCORE2. A linear regression model, adjusted for confounding factors, was used to assess the relationship between SCORE and SCORE2 with IMT. Both SCORE (estimate 1.41 p=0.02, R2=0.045) and SCORE2 (estimate 1.55 p<0.01, R2=0.015) were positively associated with IMT.
Table 1. Demographic, clinical characteristics and Ultrasound Results
Conclusion: The relationship between SCORE and SCORE2 was found to be satisfactory, indicating their adequacy for prediction plaque development. However, the predictive capacity of both scores may be further enhanced by incorporating multiplication factors. Additionally, both SCORE and SCORE2 were positively associated with IMT, but SCORE2 demonstrated a greater predictive capacity in this regard. Furthermore, the SCORE2 explained a higher proportion of the IMT variation compared with SCORE.
REFERENCES: [1] Smolen JS, Aletaha D, Barton A, et al. Rheumatoid arthritis. Nat Rev Dis Prim. 2018;4:1–23.
[2] Seoane-Mato D, Sánchez-Piedra C, Silva-Fernández L, et al. Prevalencia de enfermedades reumáticas en población adulta en España (estudio EPISER 2016). Objetivos y metodología. Reumatol Clin. 2019;15(2):90-6
[3] González Mazarío R, Fragío Gil JJ, Martínez Calabuig P, et al. Cardiovascular risk assessment with carotid ultrasound in rheumatoid arthritis. Med Clin (Barc). 2022 Nov 25;159(10):470-474. English, Spanish.
Acknowledgements: NIL.
Disclosure of Interests: None declared.