fetching data ... 
Background: Cardiovascular events (CVE) are the leading cause of mortality for patients living with systemic lupus erythematosus (SLE). Besides the traditional cardiovascular risk factors, the impact of subclinical atherosclerosis on the clinical cardiovascular risk is yet to be determined in the specific population.
Objectives: Our aim was to evaluate the association between subclinical atherosclerosis defined as the presence of an atherosclerotic carotid plaque > 1.5 mm in thickness, and the risk of future cardiovascular events in SLE.
Methods: We performed a prospective study including consecutive patients with SLE followed in our reference center. We excluded patients with a known coronary disease or symptoms suggestive of cardiovascular disease (angina, arrhythmia, congestive heart failure, stroke, and peripheral arterial disease). All patients were evaluated for carotid plaque by a single evaluator. At inclusion, we collected demographic characteristics, morphometric parameters such as body mass index (BMI) and waist circumference, disease characteristics and treatment history. The main outcome was a cardiovascular event defined as the occurrence during a 11-years follow-up of myocardial infarction, ischemic stroke or symptomatic peripheral arterial disease. We examined the association between carotid plaque and cardiovascular event onset using uni- and multivariable logistic regression using Firth’s correction for separated data.
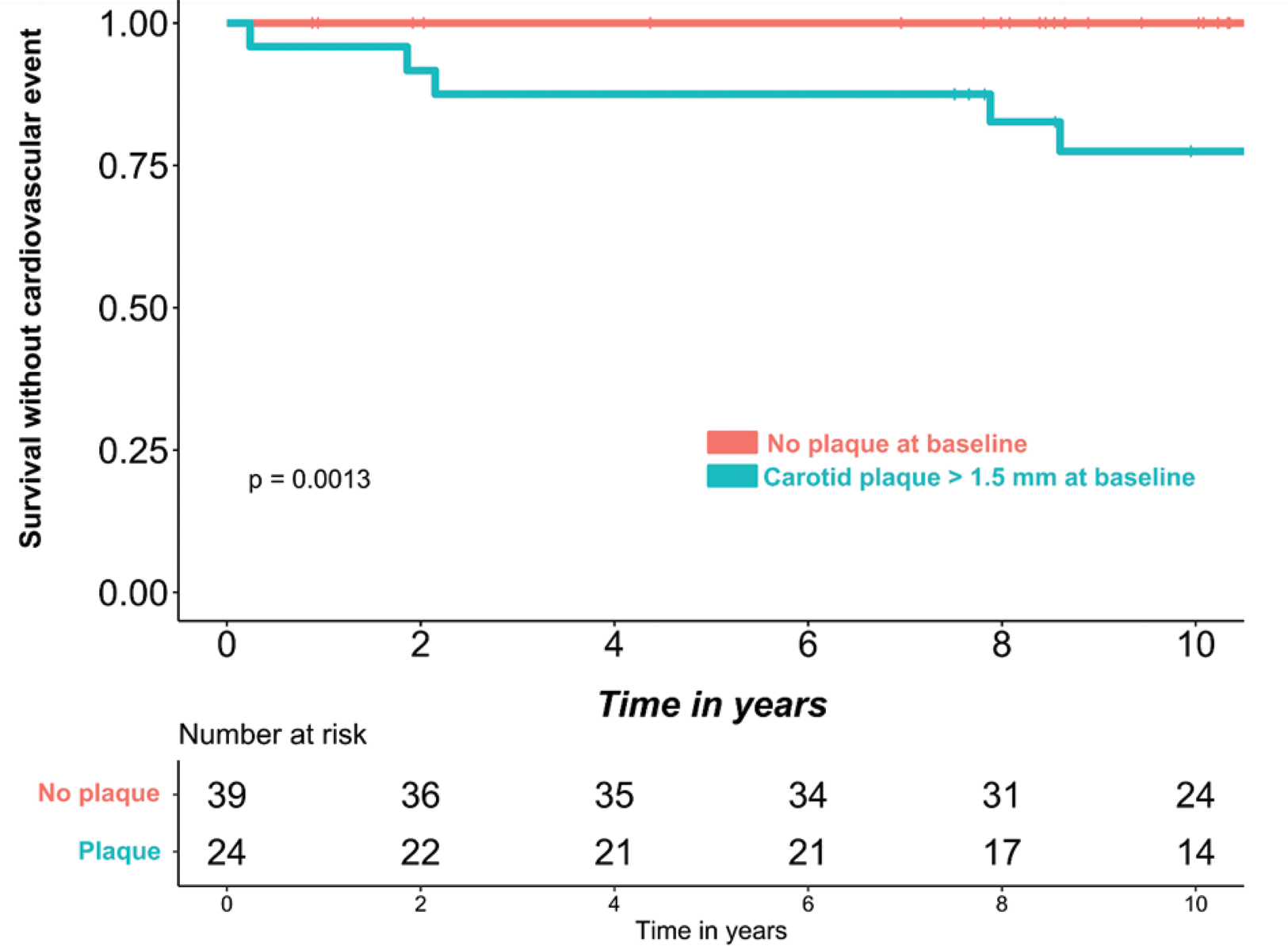
Results: We included 63 SLE patients (82.5% female), with an age of (median [1st quartile-3rd quartile]) 39 [32-44.5] years. Among them, 24 (38.1%) had a carotid plaque > 1.5 mm at baseline and 7 (11.1 %) experienced a cardiovascular event during a median follow-up of 10.7 [8.2-11.0] years. All the cardiovascular events occurred in the group of patients with a carotid plaque at baseline. The univariable analysis of the factors associated with the occurrence of a cardiovascular event are presented in Table 1 (see below). The survival without cardiovascular event in this population, according to the presence of a carotid plaque at baseline is presented as a Kaplan-Meier curve in Figure 1 (see below). In the multivariable analysis, we observed that, after adjusting for the Framingham score and the body mass index, the presence of a carotid plaque remained significantly associated with the occurrence of a cardiovascular event: odds ratio [95% confidence interval] = 15.6 [1.02, 2226]; p= 0.048.
Conclusion: Subclinical atherosclerosis defined as a carotid plaque > 1.5 mm is significantly associated with the clinical cardiovascular risk in SLE. Subclinical atherosclerosis should be regularly assessed in this population as part of the global cardiovascular risk evaluation.
Factors associated with the occurrence of a clinical cardiovascular event during follow-up.
| No cardiovascular event, n= 56 | Cardiovascular event, n= 7 | p | |
|---|---|---|---|
| Age, years | 37.00 [31.75 - 43.00] | 58.00 [49.50 - 61.50] | <0.001 |
| Female sex | 48(86) | 4(57) | 0.10 |
| BMI(kg/m 2 ) | 23.95 [20.98 - 26.37] | 25.90 [24.45 - 28.70] | 0.15 |
| Waist circumference(cm) | 90.00 [82.00 - 100.75] | 95.00 [88.50 - 106.50] | 0.3 |
| Carotid plaque > 1.5 mm | 17(30) | 7 (100) | <0.001 |
| HbA1c (%) | 5.50 [5.20 - 5.70] | 5.80 [5.20 - 5.90] | 0.4 |
| LDL cholesterol (g/l) | 0.89 [0.71 - 1.16] | 1.33 [0.98 - 1.37] | 0.11 |
| Smoking | 20 (36) | 4 (57) | 0.4 |
| Hypertension | 12 (21) | 4 (57) | 0.063 |
| Framingham score | 0.50 [0.50 - 2.00] | 7.00 [2.75 - 15.75] | <0.001 |
| Time since SLE diagnosis(in years) | 11.50 [5.75 - 16.00] | 11.00 [10.00 - 17.00] | 0.7 |
| Raynaud’s phenomenon | 17 (30) | 0 (0) | 0.2 |
| History of lupus nephritis | 29 (52) | 4 (57) | >0.9 |
| High anti-dsDNA Ig titer | 19 (34) | 3 (43) | 0.7 |
| Low C3 | 17 (30) | 3 (43) | 0.7 |
| SLEDAI | 2.00 [0.00 - 4.00] | 2.00 [1.00 - 6.00] | 0.4 |
| Lupus anticoagulant | 9 (16) | 3 (50) | 0.084 |
| Antiphospholipid syndrome | 8 (14) | 0 (0) | 0.6 |
| Hydroxychloroquine | 56 (100) | 6 (86) | 0.11 |
| Immunosuppressive drug | 41 (73) | 6 (86) | 0.7 |
| Aspirine | 5 (8.9) | 2 (29) | 0.2 |
| Statin | 13 (23) | 2 (29) | 0.7 |
Quantitative variables are presented as median [1st quartile -3rd quartile] and compared with Mann-Whitney’s test; categorical variables are presented as number(percentage) and compared with Fisher’s exact test.
Survival without cardiovascular event according to the presence of carotid plaque at baseline.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.