fetching data ... 
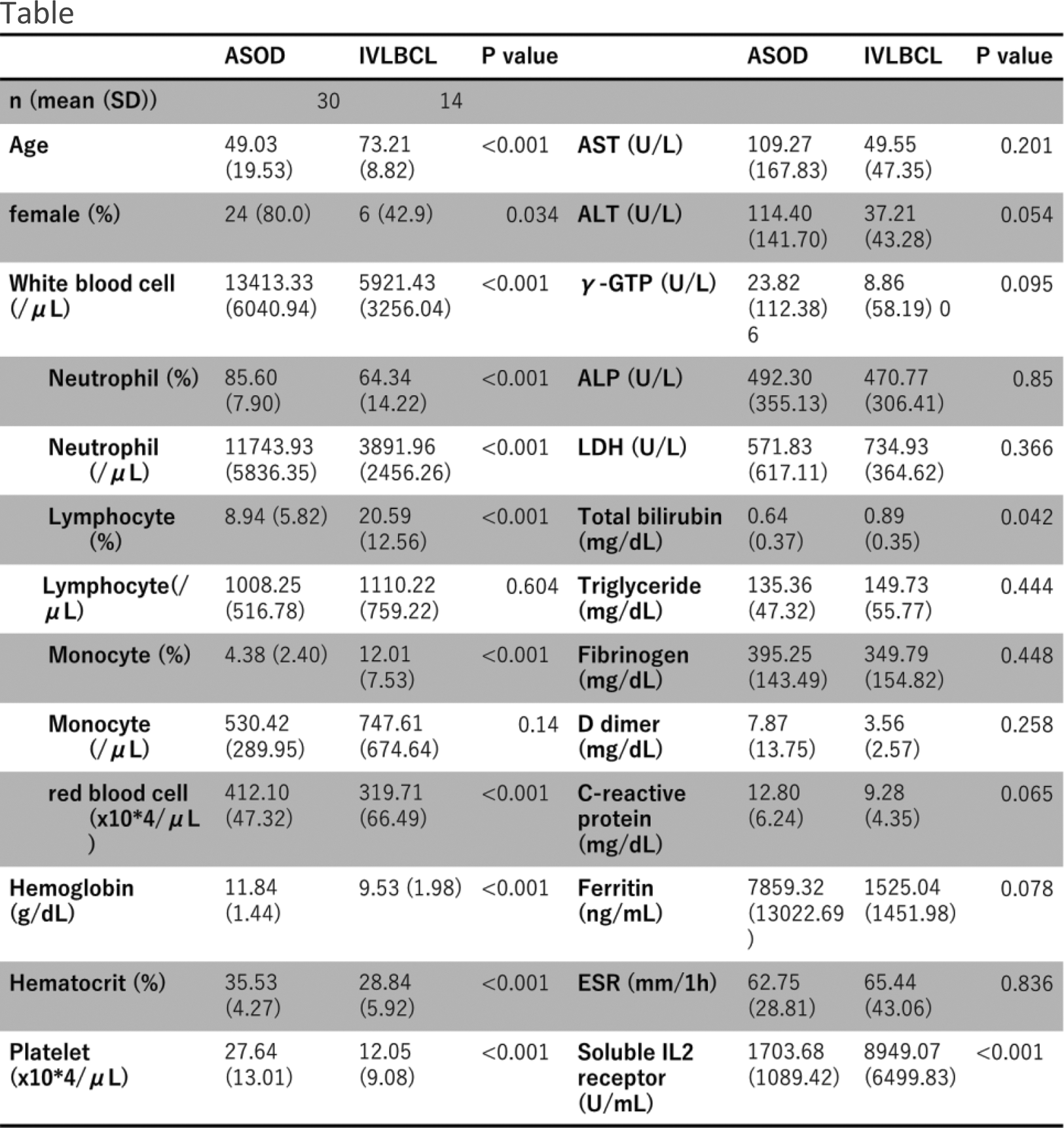
Background: In the diagnosis of the fever of unknown origins, differentiating between adult-onset Still’s disease (AOSD) and intravascular large B-cell lymphoma (IVLBCL) is challenging. Laboratory data such as soluble interleukin-2 receptors and ferritin and elevated CT attenuation values of bone marrow are used as references in the real-world clinical setting, but their usefulness has not been studied.
Objectives: This study aimed to investigate (1) factors of laboratory data and (2) CT attenuation values of the L1 trabecular and femoral bone marrow, that are possibly useful in the differentiation of these two disease.
Methods: We conducted a retrospective observational study of patients diagnosed with AOSD or IVLBCL at our hospital from April 1, 2010, to July 19, 2022. AOSD was diagnosed based on the Yamaguchi criteria, and IVLBCL was confirmed through pathological findings. Clinical symptoms and laboratory data were referenced from the medical record data. The bone marrow CT attenuation values of the lumbar and femurs were measured based on previous study [Ref1,2]. Statistical analysis was performed using R. Exploratory analysis was conducted to identify factors useful in discriminating between the two groups. For identified factors, discrimination ability was assessed using ROC curves and AUC. Sensitivity and specificity were calculated at the threshold determined by the Youden method. The statistical significance level was set at 0.05.
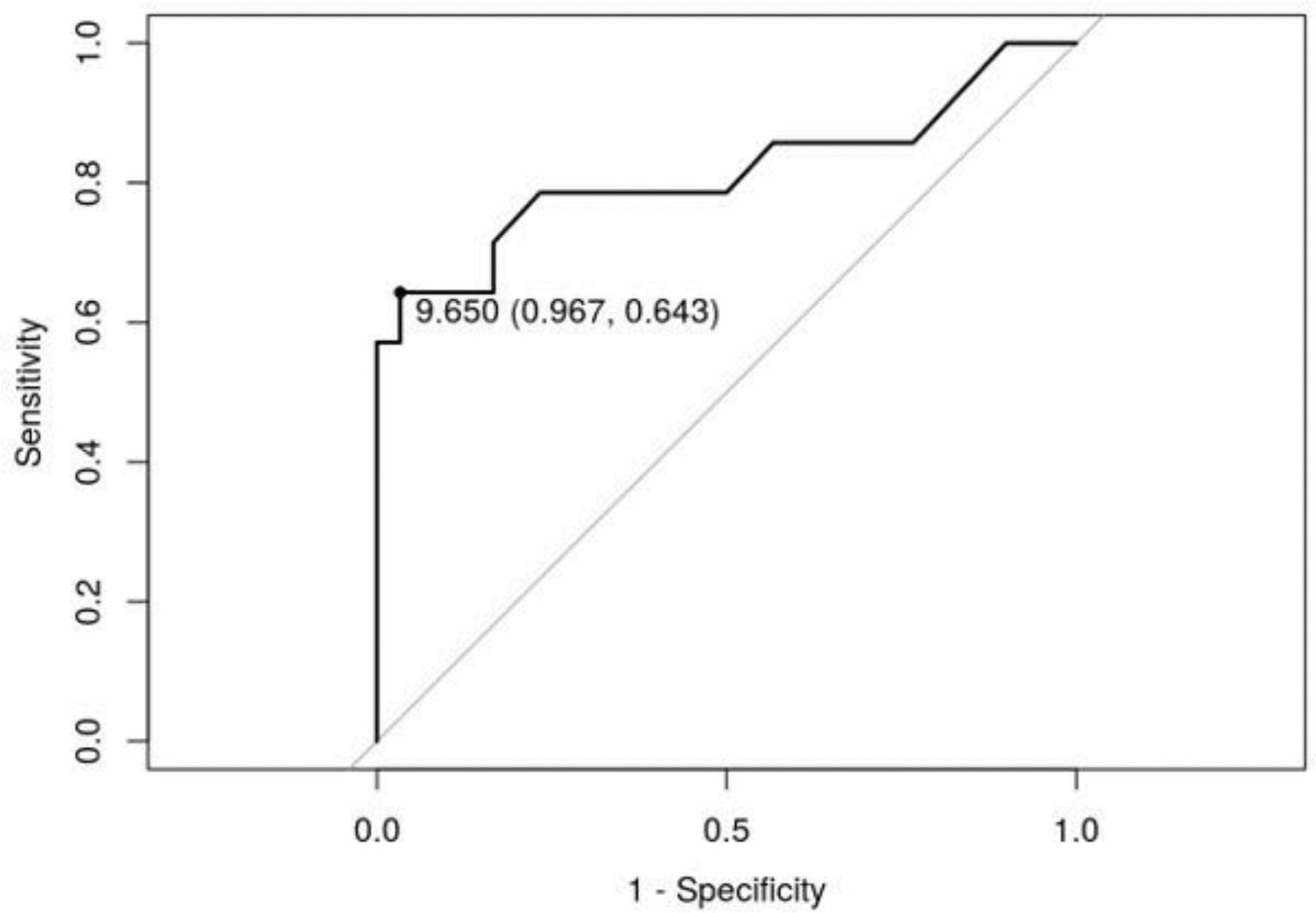
Results: This study included 30 patients of AOSD and 14 patients of IVLBCL (Table 1). There were 17 and 14 patients in the AOSD and IVLBCL groups who underwent CT, with a mean age of 57.47 and 73.21 years, respectively. (1) Significant differences were observed between the two groups in white blood cell count, monocyte fraction, soluble interleukin-2 receptor, and other parameters. No significant differences were observed in ferritin, C reactive protein, and liver function tests including LDH (Table 1). The next analysis focused on monocytes because of the increasing interest in monocytes in diseases that cause fevers of unknown origin [ref3]. Focusing on monocyte fraction (%), an AUC of 0.8143 (95% CI 0.6465-0.9821) demonstrated high discrimination ability. When the threshold was set at 9.650%, sensitivity was 64.3%, and specificity was 96.7% (Figure 1). (2) On the other hand, a no significant difference was observed in the mean CT attenuation values (HU) of the L1 trabecular and femoral bone marrow (159.05 vs 141.49(P=0.364), -16.23 vs 2.62 (P=0.16)).
Conclusion: The findings showed that a monocyte fraction (%) greater than 9.650 suggests IVLBCL in differentiation between AOSD and IVLBCL. However, it is difficult to differentiate the two diseases by CT attenuation values of the L1 trabecular and femoral bone marrow.
REFERENCES:
[1] Ishii S, Ohkawara H, Endo Y, et al. Evaluation of Computed Tomography Attenuation Value of Proximal Femoral Marrow to Diagnose and Differentiate Hematologic Malignancies, Myelofibrosis, and Aplastic Anemia. J Comput Assist Tomogr. 2021;45(6):912-918.
[2] Jang S, Graffy PM, Ziemlewicz TJ, et al. Opportunistic Osteoporosis Screening at Routine Abdominal and Thoracic CT: Normative L1 Trabecular Attenuation Values in More than 20 000 Adults. Radiology. 2019 May;291(2):360-367.
[3] Ben Mulhearn, Jessica Ellis, Tamas Somoskeoy, et al. P290 Baseline monocyte count may help make a diagnosis of giant cell arteritis: results of routinely collected audit data from two centres, Rheumatology, Volume 61, Issue Supplement_1, May 2022, keac133.289.
Table 1.
Acknowledgements: NIL
Disclosure of Interests: None declared.