fetching data ... 
Background: The emergence of immune checkpoint inhibitors (ICI), a type of immunotherapy, has revolutionized the treatment of many malignant neoplasms. However, immune-mediated adverse events have often been reported. Among them, ICI-related myositis is one of the most serious and difficult-to-treat complications.
Objectives: To describe the clinical features, management and outcome of patients with ICI-related myositis.
Methods: National Observational multicenter study from clinical practice of ICI-related myositis reported between 2016 and 2023. We reviewed demographic, clinical features, treatment and outcomes. In addition, we conductress a literature review in PubMed, Embase and the Cochrane library from their inception up to 31 December 2023.
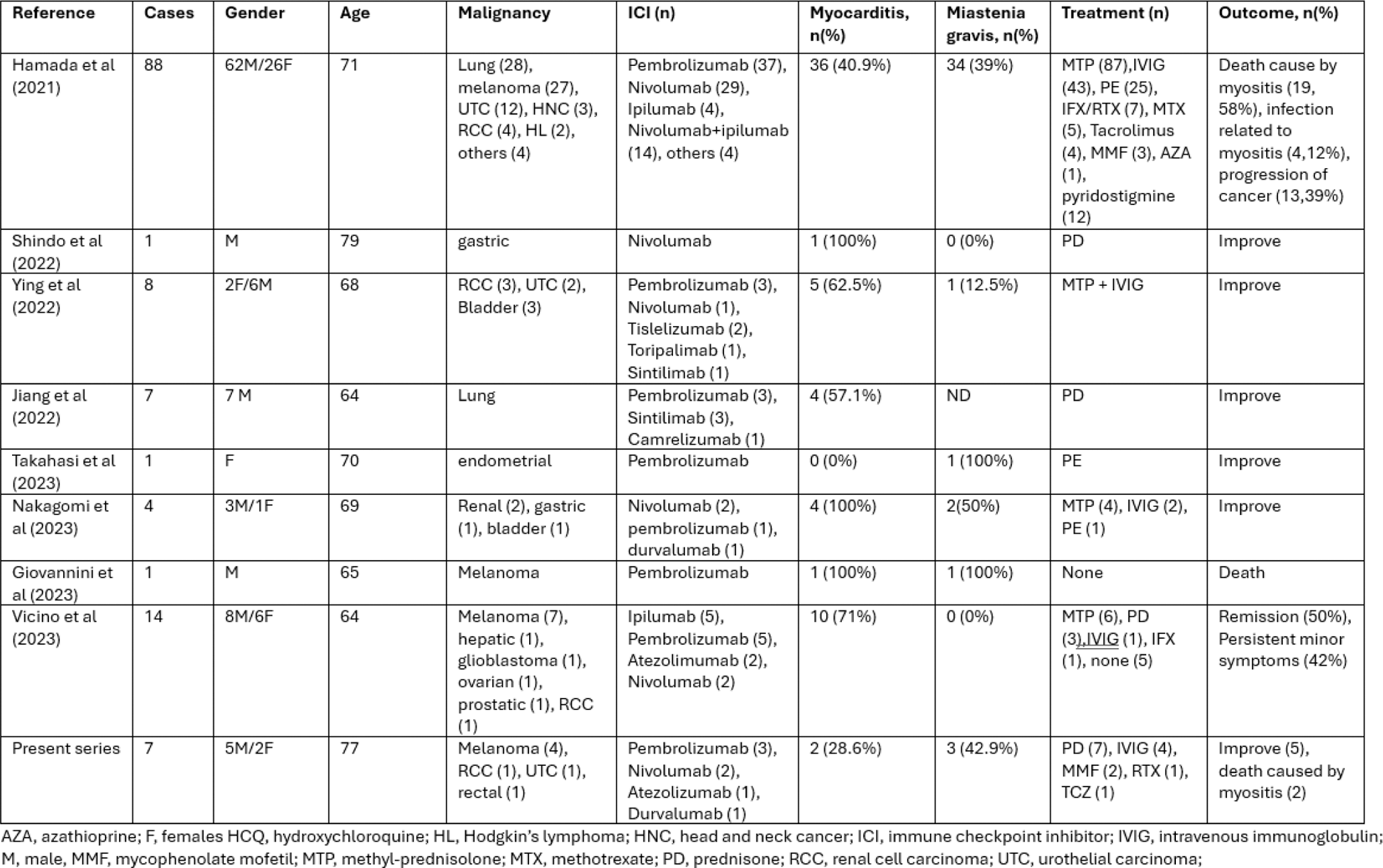
Results: We present 7 patients (2 women, 5 men), mean±SD age 77.1± 7.0 years, with ICI-related myositis. The most common malignancy was melanoma (n=4), followed by renal cell carcinoma (n=1), urothelial carcinoma (n=1) and rectal cancer (n=1). Patients received the following ICI therapy: pembrolizumab (n=3), nivolumab (n=2), atezolizumab (n=1) and durvalumab (n=1). Myocarditis and miastenia gravis (MG) were also present in 28.6% and 42.9% of patients, respectively. Other adverse events included: hepatitis (n=3), pneumonitis (n=1), encephalitis (n=1), thyroiditis (n=2), diarrhea (n=1) and toxicoderma (n=1). A marked elevation of CK was observed in all patients (median[IQR]: 3023[1990-3500] U/L). Treatment consisted of ICI discontinuation and immunosuppressive agents: all received oral glucocorticoids, IVIG (n=4), mycophenolate (MMF) (n=2), rituximab (RTX) (n=1), tocilizumab (TCZ) (n=1). Most of the patients (5/7) improved, two patients died. In the literature review (Table 1), we found 124 patients (31 women/93 men, mean±SD 69.7±5.1 age). The most frequent malignancy was melanoma and the most common ICI pembrolizumab. The prevalence of myocarditis and MG varies widely among the different studies. Therapeutic strategies included glucocorticoids in almost all patients, plasma exchange (n=26), IVIG (n=60), conventional DMARDs [MTX (n=5), MMF (n=5), AZA (n=1)] and biologics [IFX (n=8), RTX (n=8), TCZ (1)]. Most of patients improved, but death related to myositis were reported in 20 (17.7%) of patients.
Conclusion: Our study highlights that ICI-related myositis is a severe adverse event of ICI that needs early treatment including ICI discontinuation and immunosuppressive therapy.
Table 1.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.