fetching data ... 
Background: Immunosenescence (IS) is a global remodeling of immune functions that has been first described with aging. It is also associated with infectious diseases and cancer. Circulating immunosenescent (IS) T-cells are observed in more than 25% of the patients with advanced non–small cell lung and correlates with lack of benefit from immune checkpoint inhibitors. The mechanisms leading to IS are still only partially understood and IS is poorly described in Immune mediated inflammatory diseases (IMIDs). Chronic inflammation is a potential driver.
Objectives: Here we sought to assess the level of circulating IS CD8 T-cells (T 8 sen) in patients with IMIDs and prospectively assess the effect of anti-TNF.
Methods: We have included 25 patients with rheumatoid arthritis (RA), 22 patients with spondyloarthritis (SA) and 20 patients with Sjögren disease (Sjo). IS T-cell have been assessed by flow-cytometry on fresh whole blood. Senescent immune phenotype (T 8 sen) was defined by the percentage of CD28- CD57+ KLRG1+ among circulating CD8+ T cells. Anti-TNF naïve patients with RA and SA were evaluated at baseline and 3 months after anti-TNF initiation. Responders were defined as patients still under the same anti-TNF treatment at 12 months. IFNα2a, IFN-β, IFNγ, IFNλ1, IP-10, IL-6 and TNF were measured in sera in all the patients at baseline using MSD technology. CMV serology was assessed using IgG Elisa. Associations between SIP and categorical or continuous variables were performed by logistic regression/Fisher exact test or Mann–Whitney test, respectively.
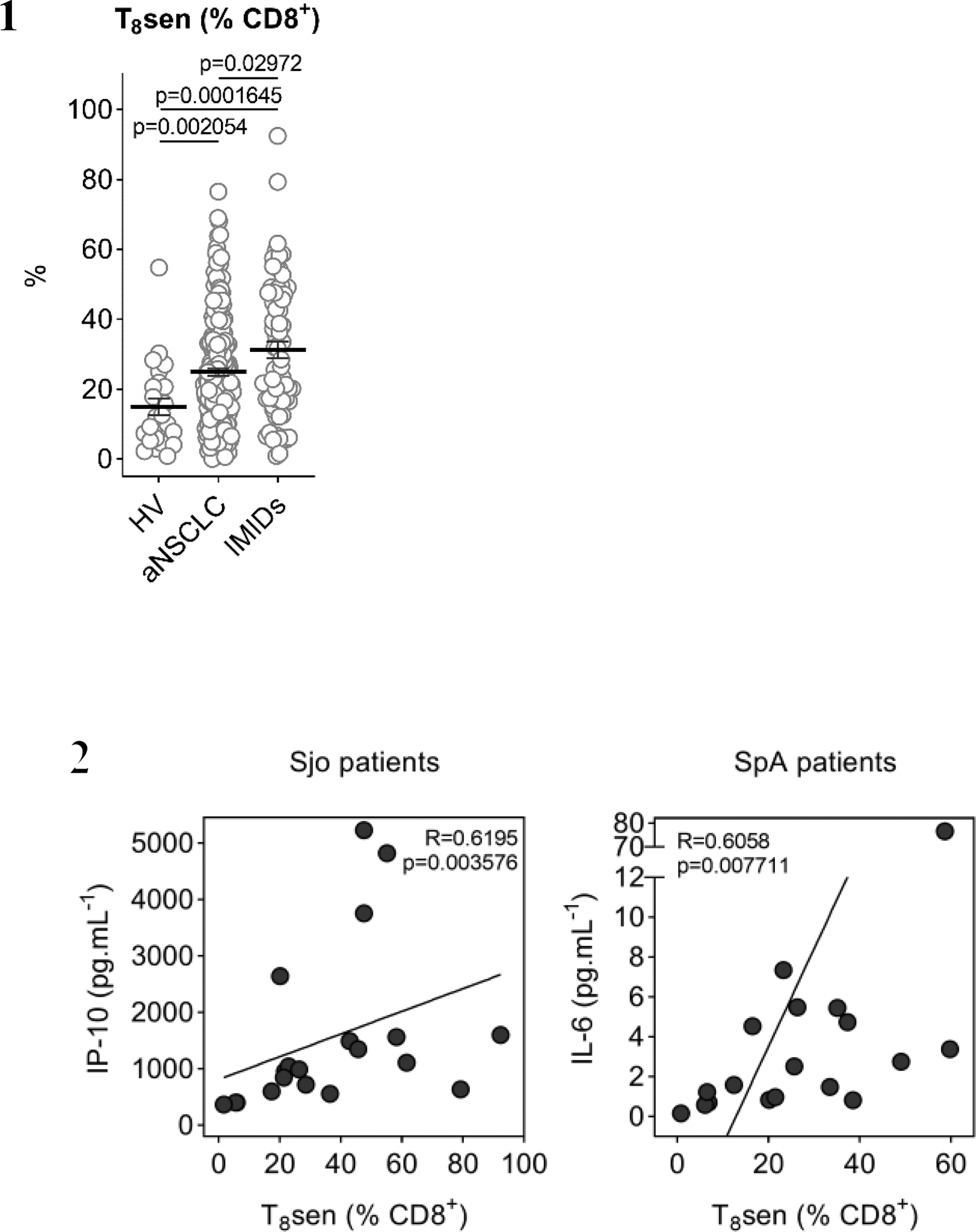
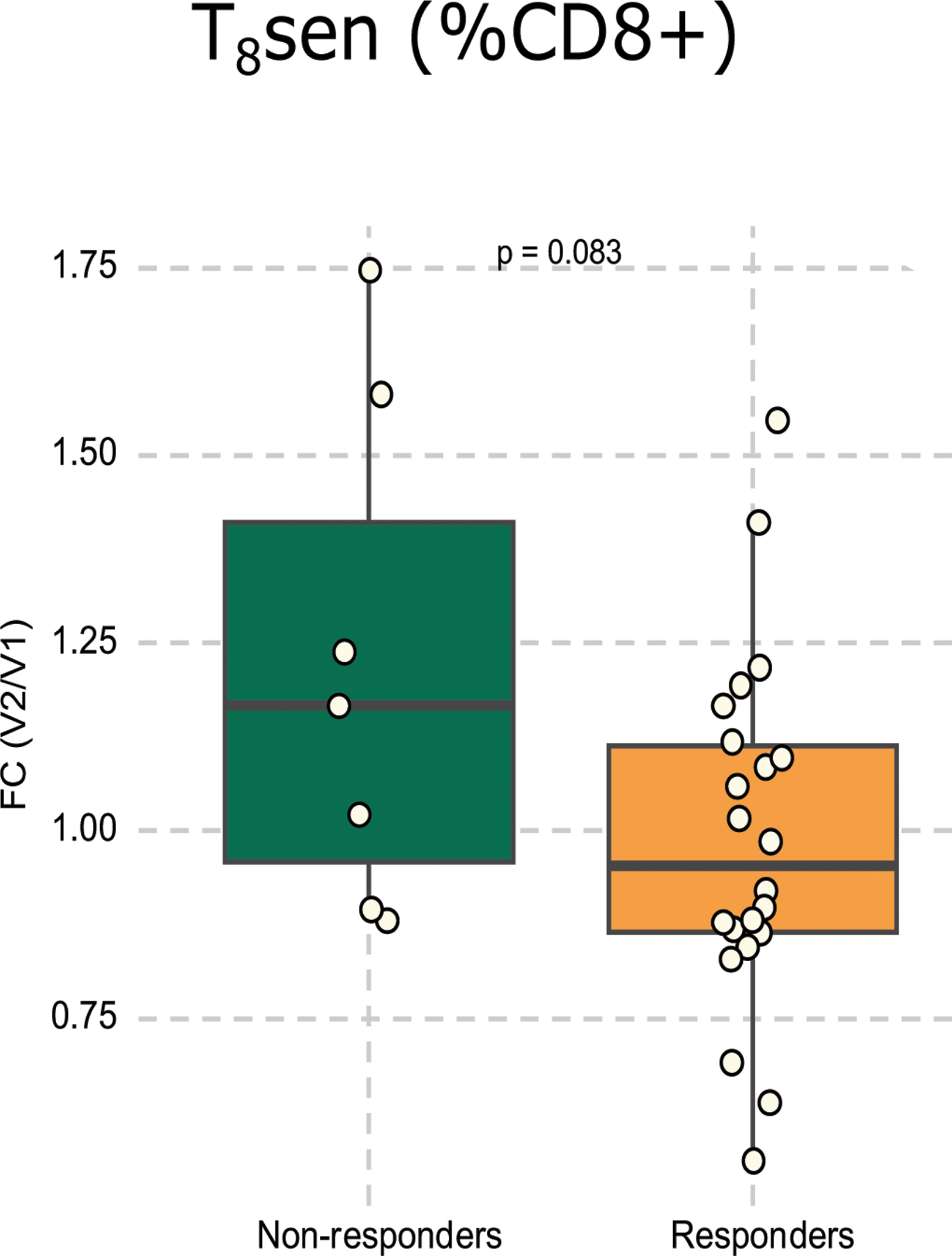
Results: Patients with IMIDs presented a high level of circulating IS T-cells (Figure 1). The median level of T 8 sen was 26.31% in IMIDS patients compared to 23.8% in cancer (p=0,03) and 15% in healthy controls (p<0,01). Among the three IMIDs, T 8 sen tended to be higher in patients with Sjo. We did not observe any significant correlation between T 8 sen and disease characteristics or activity at baseline. T 8 sen were higher in CMV seropositive patients. Interestingly, we observed a significant correlation between IP-10 and T 8 sen in Sjo patients and between IL-6 and T 8 sen in SpA patients (Figure 2 top panel). Importantly, anti-TNF treatment did not diminish T 8 sen level in RA and SpA patients at 3 months but T 8 sen tended to increase in anti-TNF non-responders (1,67-fold increase) and were stable in responders (0,95-fold change for responders p=0,083 Figure 2 lower panel)
Conclusion: Patients with IMIDs exhibit a high level of T 8 sen that exceeds the levels observed in cancer. This is positively associated with IP-10 in Sjo patients and IL-6 in SpA patients. This senescence is not diminished globally with anti-TNF but tends to increase in non-responders. Since CD8 T-cell senescence has been associated with diminished cancer immunosurveillance it warrants further investigation in IMID patients who are at high risk of cancer.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.