fetching data ... 
Background: Systemic sclerosis (SSc) and ANCA associated vasculitis (AAV) are rare autoimmune disorders both characterized by vascular injury. Although ANCA have been detected in about 10% of SSc patients, only few cases of SSc patients with clinically overt AAV have been reported. Herein, we present the case of a SSc patient who developed acute renal failure due to AAV glomerulonephritis.
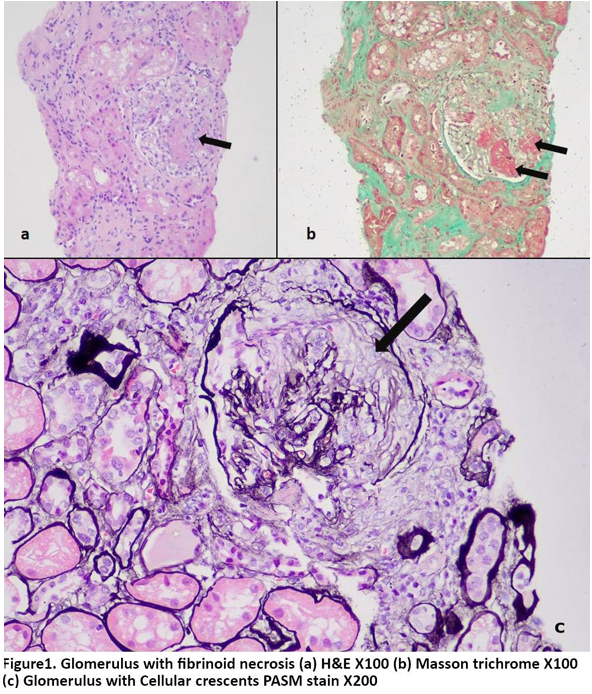
Case presentation: A 74-year-old female, with history of hypertension and nephrolithiasis, was admitted with symptomatic severe anemia (Hb:6.2g/dl). Upper GI endoscopy revealed gastric antral vascular ectasias, which were treated with 4 sessions of argon plasma coagulation. There was no evidence of cirrhosis or portal hypertension. Nine months later, she had raised Cr =1.6mg/dl (baseline 0.9), microscopic hematuria with abnormal RBCs, and proteinuria of 2gr/24h. US reported normal size kidneys without microlithiasis or obstruction and no arterial stenosis. High titer anticentromere ANA (1/1280) with ACA >200 (NV <20 RU/ml) along with p-ANCA (1/320) and MPO 148 (<20 RU/ml) were present. Clinical examination was unremarkable except for a minor sclerodactyly. The patient described Raynaud’s phenomenon since she was young. Capillaroscopy showed dilated capillaries and presence of capillary hemorrhages. No signs of scleroderma renal crisis were observed. Kidney biopsy revealed pauci- immune glomerulonephritis with necrosis and crescents. She received pulses of corticosteroids and cyclophosphamide which improved kidney function with resolution of proteinuria and hematuria.
Learning points for clinical practice: SSc can cause rapidly progressive renal failure, mainly due to scleroderma renal crisis. In patients with worsening renal function and active urine sediment, kidney biopsy is of paramount importance, even when history provides other compatible causes. Coexistence SSc with AAV is extremely rare and requires intense immunosuppression. Awareness of this association could facilitate earlier diagnosis and appropriate management to reduce damage.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.